Fig. 20.1
Schematic diagram showing types of colorectal resection. (a) Ileocecal resection, (b) right hemicolectomy, (c) left hemicolectomy, (d) Hartmann procedure, (e) anterior resection, (f) abdominoperineal resection (APR), (g) total colectomy, (h) restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA)
20.4.2 Usual Imaging Finding of the Postoperative Colon: Presacral Fluid Collection and Soft Tissue
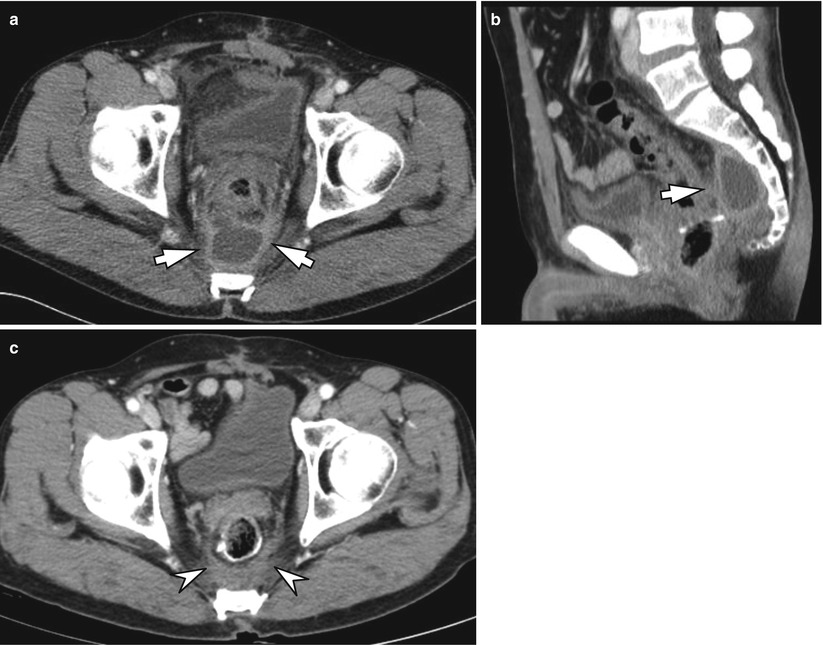
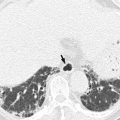
Fig. 20.2
Usual presacral fluid collection and soft tissue after rectal surgery. On axial (a) and sagittal (b) CT images taken 3 months after low anterior resection for rectal cancer, a fluid collection (arrows) confined in the presacral space is seen. (c) On follow-up CT, the presacral fluid has resolved and soft tissue (arrowheads) remains, which has been stable for 7 years (not shown)
20.4.3 Usual Imaging Finding of the Postoperative Colon: Posterior Displacement of Pelvic Organs
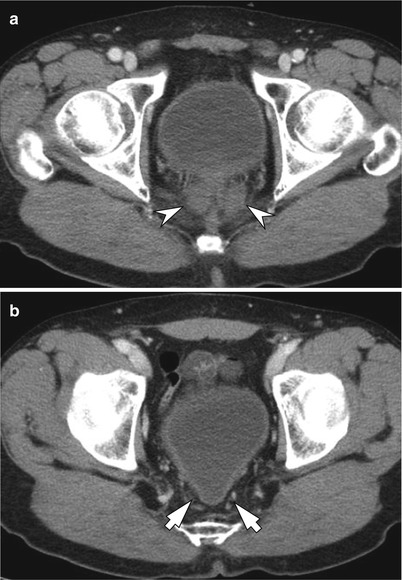
Fig 20.3
Usual posterior displacement of pelvic organs after rectal surgery. (a, b) Axial CT images obtained after abdominoperineal resection show expected posterior displacement of seminal vesicles (a, arrowheads) and the urinary bladder (b, arrows)
20.4.4 Postoperative Complication: Parastomal Hernia

Fig. 20.4
Parastomal hernia as a wound complication after colorectal surgery. On axial CT image of a patient who had undergone abdominoperineal resection, there is parastomal hernia of the small bowel at the sigmoid colostomy site (arrowheads)
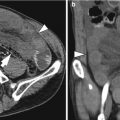
20.4.5 Postoperative Complication: Anastomotic Leak
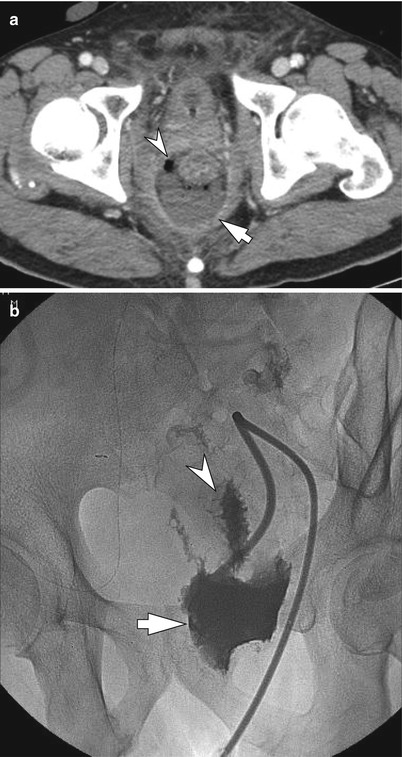
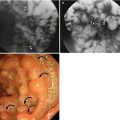
Fig. 20.5
Anastomotic leak after low anterior resection. On axial CT image (a) taken on the third postoperative day in a patient who had undergone low anterior resection for rectal cancer, there are collections of fluid (arrow) and gas bubbles (arrowhead) around the colonic anastomosis site. Percutaneous drainage was performed for this perianastomotic fluid collection as it was considered to be a fever focus. On the fluoroscopic image of tubogram (b) obtained on the twelfth postoperative day, the contrast had filled the perianastomotic abscess cavity (arrow) and also the colonic lumen just above the anastomotic site (arrowhead) confirming the presence of anastomotic leak
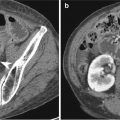
20.4.6 Postoperative Complication: Anastomotic Leak with Peritonitis and Intraperitoneal Abscess
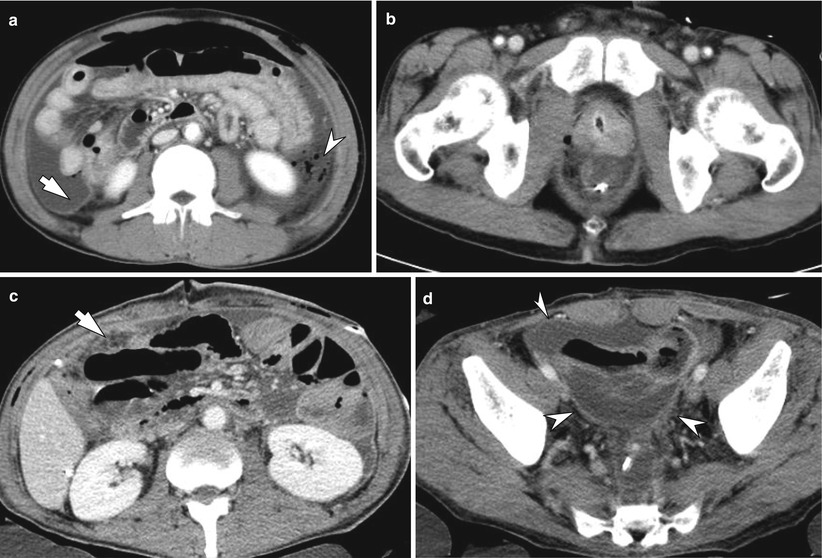
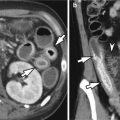
Fig. 20.6




Anastomotic leak with peritonitis and fecal spillage. Axial CT images (a) obtained on the first postoperative day in a 49-year-old man who had undergone ultralow anterior resection for rectal cancer demonstrate substantial amount of ascites and peritoneal thickening (arrow) suggesting peritonitis. There are also signs of bowel perforation including pneumoperitoneum of considerable amount and collections of mottled gas bubbles (arrowhead) suggesting fecal spillage. However, only minimal gas bubbles could be seen around the colonic anastomotic site (b). As the patient showed signs of septic shock, emergency laparotomy was performed immediately after the CT, which revealed anastomotic dehiscence and peritonitis with intraperitoneal feces. On the axial CT image acquired 5 days later, findings of generalized peritonitis have become more evident with diffuse peritoneal thickening and dirty infiltrations in the omentum (c, arrow). There is loculated fluid collection with thickened enhancing wall (arrowheads) suggesting intraperitoneal abscess in the pelvic cavity (d)
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
