6 Radiologic Anatomy of the Nasal Cavity and Paranasal Sinuses
Conventional radiography (plain film) of the paranasal system and other parts of the skull is frequently used as a screening tool in the diagnosis of sinusitis, but has limited value for detailed evaluation due to superimposition of structures.
For more accurate preoperative evaluation and use during surgery, computed tomography (CT) is the preferred tool to visualize anatomic borders and to detect pathology in the paranasal system. Although CT does not always clearly differentiate between soft-tissue processes and secretions, it provides crucial information about disease localization and integrity of the osseous structures.
Magnetic resonance imaging (MRI) enables better discernment of the characteristics of soft-tissue disease and the relation to other anatomic structures, as well as spread to and invasion into these structures. Detailed information is provided about the intracranial compartments as well as the intraorbital structures. Examples of MRI are shown and discussed in Chapter 5.
In conventional radiography, the Caldwell view and Waters view are the most commonly used projections; these are complementary to each other.
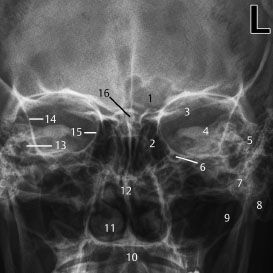
Fig. 6.1 Caldwell view
1 Left frontal sinus, right side aplasia
2 Ethmoid sinus
3 Planum sphenoidale
4 Superior aspect of the petrous bone
5 Pneumatized and aerated mastoid cells
6 Foramen rotundum (infraorbital canal)
7 Zygomatic arch (better seen on Waters view)
8 Mastoid apex
9 Maxillary sinus
10 Maxilla
11 Inferior turbinate
12 Nasal septum
13 Cochlea
14 Innominate line of the greater wing of the sphenoid
15 Lamina papyracea
16 Crista galli

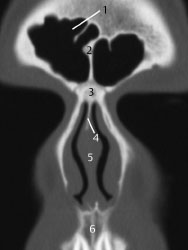
Fig. 6.2 Waters view
1 Frontal sinus
2 Frontal recess
3 Supraorbital nerve canal
4 Orbital floor
5 Maxillary sinus
6 Sphenoid sinus
7 Intersphenoidal septum

Fig. 6.3 Waters view. Waters view of a 7-year-old child. The frontal sinuses are not yet pneumatized. In the region of the maxillary sinus, several unerupted teeth are present, which limit the surgical procedures that can be carried out in this area.
Evaluation Points for CT of the Nasal Cavity and Paranasal Sinuses
Although most of the below-mentioned points of evaluation might also be evaluated on plain films, CT will demonstrate much more detail on bony outlines and contents. Systematic evaluation is best done in an anteroposterior sequence, starting with the coronal slices followed by a craniocaudal sequence of axial slices. In both sequences, the evaluation starts with the less complex slices. The paranasal sinuses as well as the remaining structures are systematically and bilaterally screened according to the points mentioned below. Although a clinical description will end up being longer, it is always worth looking at both sides in the evaluation, even in cases without pathology.
Frontal Sinus
• Presence, extension, and degree of pneumatization, bony outlines.
• Contents: septal structures, aeration or opacification of the sinus.
• In case of opacification: characteristics such as calcifications.
• Frontal recess: patency and opacification.
Ethmoid Sinus
• Degree of pneumatization, bony outlines.
• Opacification: diffuse, localization (anterior/posterior).
• Ethmoid roof: appearance, height, and left/right differences.
• Ethmoid bulla: morphology, degree of caudal extension.
• Lamina papyracea.
Infundibulum
• Patency, morphology of the uncinate process.
• Obstruction by a caudally extended ethmoid bulla, opacities.
Maxillary Sinus
• Degree of pneumatization, bony outlines, tooth elements, any fistulas from the maxilla.
• Morphology of the bony canal containing the infraorbital nerve.
• Presence of retention cysts and their relation to the natural ostium, degree of obstruction, opacifications and their characteristics.
• Degree of pneumatization, bony outlines, opacification.
• Optic and internal carotid canals, foramen rotundum, pituitary fossa.
Remaining structures
• Nasal septum: deviations, septal spine or spur, crista galli.
• Nasal turbinates: morphology, pneumatization, obstructive effects.
• Cribriform plate, skull-base height differences, lacrimal duct, intraorbital pathology.
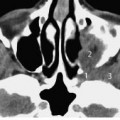
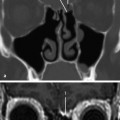
Radiologic Anatomy on Coronal CT Slices in an Anteroposterior Sequence
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


