Fig. 4.1
HCC: (a, b) contrast-enhanced CT reveals arterially enhancing lesion in the lateral segment, i.e. segment III (a), and wash out on porto-venous phases (b). On MRI (c–e), a well-defined T2 hyperintense signal lesion (c) which shows rapid wash in on the arterial phase (d) and wash out on porto-venous phase (e). These imaging findings are classical for hepatocellular carcinoma
The typical pattern of enhancement on both CT and MRI scan would be rapid arterial enhancement and wash-out on porto-venous phases and delayed enhancing capsule due to fibrous nature [11]. Arterio-portal shunting is also one of the characteristic features [12]. HCC can cause spontaneous haemorrhage, and surface HCC can rupture leading to hemoperitoneum. On MR imaging it will be hypointense on T1-weighted imaging. It can be hyperintense due to fat, protein or blood content within. On T2 these lesions would be hyperintense with restricted diffusion. Small HCC are <2 cm in size and have classical features, whereas large HCC will not show classical enhancement pattern and will have haemorrhage and necrosis. HCC are known to cause portal vein tumour thrombus which on imaging will enlarge the portal vein, cause arterial enhancement and neovascularity. HCC can have scar, calcification, fat and blood and can be cystic. They can be solitary, well-defined, multiple or diffuse [13].
Fibrolamellar carcinoma occurs in younger patients without underlying liver disease. These on imaging appear as large well-defined lobulated tumours with central scar, calcifications and heterogeneous enhancement [14, 15]. On MRI, these are hypointense on T1-weighted and heterogeneously hyperintense on T2-weighted images [15]. The scar is hypointense on T2 and shows delayed enhancement on post-contrast.
LI-RADS—The Liver Imaging Reporting and Data System is developed by the American College of Radiology with the aim to reduce variability in lesion interpretation, standardizing of the reporting content, improving communication with the clinician and decision-making, outcome monitoring, performance auditing, quality assurance and research [16].
Biopsy is indicated for the nodules which are >1 cm and do not show characteristic pattern on imaging [17–19].
BCLC staging is widely used for HCC since it combines predictor of survival and treatment options.
BCLC staging is widely used for HCC since it combines predictor of survival and treatment options. In radiological stage B of BCLC which is an intermediate group, say, one lesion more than 3 cm or more than three lesions irrespective of size, the best option is transarterial chemoembolization (TACE) [20].
Other liver lesions are discussed in the table.

Liver tumours | Imaging findings |
|---|---|
Metastases | On imaging these will be solitary or multiple and well defined which may be hypervascular as in renal cell carcinoma, carcinoid tumour, malignant adrenal tumours, thyroid carcinoma, pancreatic islet cell tumours, NET, sarcomas and melanomas. Calcifications can occur in mucinous colon carcinoma and gastric, breast, renal, carcinoid and lung carcinomas. On MR, these will be hypointense on T1 and hyperintense on T2, except for haemorrhagic lesions which have T1-hyperintense lesions (Fig. 4.2) |
Biliary cystadenocarcinoma | On CT these are well-defined intrahepatic masses, which are cystic, with enhancing wall, mural, septal nodules or soft tissue papillary projections on contrast study. On MRI, T1 and T2 show variable signal intensity but will have contrast enhancement similar to CECT |
Haemangioendothelioma | Middle age, predominant in females. Lesions are multiple which coalesce to form masses, capsular retraction; tumour enhances peripherally. On MR, hypointense on T1 and homogenous or heterogeneously hyperintense on T2 with peripheral enhancement |
Angiosarcoma | Variable enhancement which may be nodular and irregular; may have areas of haemorrhage within. On MR, large mass which may be hypo or hyper due to haemorrhage on T1 and heterogeneously hyperintense on T2 and may show heterogeneous and progressive enhancement on post-contrast |
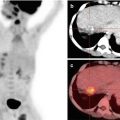
Fig. 4.2
Metastasis: Sixty-year old gentleman with pain in abdomen and mild constipation for 3 months. USG reveals multiple hypoechoic lesions. The above PET/CT images reveals FDG avid lesion in the hepatic flexure (a) which on corresponding CECT reveals circumferential heterogeneously enhancing thickening (b). Also FDG avid hepatic lesions (c) which on CECT (d) shows non-enhancing liver lesions. Colonoscopy and biopsy were done which reveal adenocarcinoma
For MRI contrast agents for the liver. There are four types:
- 1.
Extracellular agents
- 2.
Reticuloendothelial agents
- 3.
Hepatobiliary agents
- 4.
Blood pool agents
- 5.
Combined agents
Extracellular agents —Mechanism depends on the gadolinium, which has seven unpaired electrons and is highly paramagnetic resulting in shortening of the T1 and T2 relaxation times of adjacent water protons and causing signal enhancement at T1-weighted imaging and loss of signal at T2-weighted imaging [21, 22]. It is used in lesion detection, characterization and liver vascular anatomy.
Reticuloendothelial agents —Superparamagnetic iron oxides, e.g. ferucarbotran, are currently used as reticuloendothelial agents. They are phagocytosed by macrophages throughout the body but are entrapped by Kupffer cells [23]. They act as negative contrast agent, and due to their superparamagnetic properties, they cause T2 and T2 * shortening [24]. It is used with liver tumours since they are deficient in Kupffer cells and do not exhibit SPIO particle uptake. So after injection of SPIO, the tumour will appear hyperintense since the background is suppressed [25].
Hepatobiliary agents —As they have five unpaired electrons, paramagnetic agents are taken by functioning hepatocytes and excreted in the bile [26]. It shortens T1 and T2 relaxation times of water protons. It is used for characterization of hepatocellular and non-hepatocellular masses since these agents are taken by the hepatocytes (e.g. HCC, focal nodular hyperplasia, hepatic adenoma) and surveillance of the liver for metastasis and functioning of biliary system.
Combined agents —Gadobenate dimeglumine has the property of an extracellular, hepatobiliary and blood pool agent. It is used for HCC, focal nodular hyperplasia and non-hepatocellular lesions, adenoma, metastasis and haemangioma [26].
Cholangiocarcinoma is the second most common malignancy of the biliary system. According to its anatomical origin, it is classified as intrahepatic, hilar or extrahepatic [27].
Intrahepatic CC is an adenocarcinoma that arises from the epithelium of the small intrahepatic bile ducts. Predisposing factors are primary sclerosing cholangitis, Clonorchis sinensis infestation, thorium dioxide exposure and congenital biliary anomalies. They are further macroscopically divided into mass form, periductal or intraductal growth. Clinical presentation depends on the location of the mass; peripheral masses are diagnosed late as they cause pain only in late stage where central hilar will cause painless jaundice early. On CT it presents as having a low attenuation mass with incomplete peripheral arterial enhancement that becomes iso- or hypodense on porto-venous phase. Capsular retraction is seen due to fibrosis. There can be ductal dilatation and mural thickening seen in peripheral intrahepatic ducts [28]. On MRI they appear hypointense on T1 and hyperintense on T2. Central area may be hypo or hyper due to fibrosis, mucin or oedema. It shows mild to moderate enhancement with progressive centripetal fill-in of the contrast on delayed phases [29]. On USG it shows solid heterogeneous echotexture mass (Fig. 4.3).

Fig. 4.3
Cholangiocarcinoma: Fifty-eight-year old male with pain in abdomen and progressive painless jaundice since 2 months. CECT done outside reveals mass in the left hepatic duct with periportal lymph nodes. MRI abdomen (a–c) with MRCP (d) done which shows ill-defined altered signal intensity mass lesion in the left hepatic duct () extending into the common hepatic duct which shows delayed progressive enhancement, atrophy of the left lobe of liver and mild IHBR dilatation in both lobes. These features are s/o cholangiocarcinoma. MRCP (d) reveals stricture () involving the left hepatic duct, confluence and just extending into the right anterior and posterior ductal system s/o type IV block. PTC gram (e) done which reveals multiple segmental block s/o type IV block
Peripheral CC are primary biliary tumours arising between the right and left and the common hepatic duct up to the cystic duct insertion and also known as Klatskin’s tumours [30]. On CT/MR, it will show focal mural thickening with luminal obliteration and peripheral ductal dilatation, periductal thickening with mass, focal liver atrophy, vascular encasement, lymph nodal involvement and distant metastasis.
Distal CC originates between the insertion of the cystic duct in the extrahepatic channel and the ampulla of Vater. On cross-sectional imaging, tumour will show soft tissue density with delayed enhancement and abrupt cut-off and infiltrative thickening of bile duct wall.
4.1 Gall Bladder Carcinoma
It is the most common biliary malignancy worldwide. Most of the patients are diagnosed in late stages due to vague symptoms. Predisposing factors include cholelithiasis, porcelain gall bladder, choledochal cyst, congenital cystic dilatation of biliary tree, anomalous pancreatico-biliary junction and low cystic duct insertion and primary sclerosing cholangitis. Clinical presentation includes abdominal pain, fever, weight loss and jaundice [31].
There are three patterns of gall bladder carcinoma :
- 1.
Mass obliterating the gall bladder lumen
- 2.
Focal or diffuse gall bladder wall thickening
- 3.
Intraluminal polypoidal mass [32]
Radiological features in:
- 1.
Mass-forming lesion—On USG it shows heterogeneously hypoechoic mass filling partially or completely. On CT it will show heterogeneously enhancing mass lesion. There may be presence of calcification within the mass or calculi within the gall bladder lumen [33]. On MRI it will show T1 hypointensity and T2 moderate hyperintensity. Similar contrast enhancement is seen as that of CT. CT helps to demonstrate involvement of the hepatic flexure of the colon or regional adenopathy. Primary tumour can infiltrate along the bile ducts and biliary system.
- 2.
Focal or diffuse wall thickening—On cross-sectional imaging, it will show asymmetrical, irregular or extensive thickening showing heterogeneous enhancement. It needs to be differentiated from acute and chronic cholecystitis, xanthogranulomatous cholecystitis and adenomyomatosis.
- 3.
Intraluminal polypoidal mass—It is a mass larger than 1 cm in diameter which is immobile upon changing position on USG.
CT scan is for preoperative staging and MRCP for bile duct and vascular invasion.
4.2 Pancreatic Carcinoma
Pancreatic adenocarcinoma is the most common malignancy of the pancreas.
These tumours are located 60–70% in the pancreatic head, 10–20% in the pancreatic body and 5–10% in the pancreatic tail. They present with pain in abdomen, weight loss and jaundice.
On ultrasound it would be a poorly defined heterogeneous hypoechoic mass. Other indirect signs include dilatation of the pancreatic duct, biliary duct dilatation or both (double duct sign). On CT it will be hypoenhancing mass; tumour in the pancreatic head causes dilatation of CBD and main pancreatic duct, whereas tumour in body of pancreas will cause upstream MPD dilatation. Cross-section imaging will also demonstrate vascular invasion, thrombosis and collateral vessels [34]. On MR it is hypointense on T1 and T2 due to scirrhous fibrotic nature and shows restricted diffusion. Metastases are frequently seen in liver and peritoneum (Fig. 4.4).

 Management of Hepatobiliary and Pancreatic Malignancies
Management of Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies: Epidemiology, Clinical Presentation, Diagnosis, and Staging
Hepatobiliary and Pancreatic Malignancies: Epidemiology, Clinical Presentation, Diagnosis, and Staging
 PET/CT in Pancreatic Malignancies
PET/CT in Pancreatic Malignancies
 Pathology of Hepatobiliary and Pancreatic Cancer
Pathology of Hepatobiliary and Pancreatic Cancer
 PET/CT in Gall Bladder and Biliary Tract Malignancies
PET/CT in Gall Bladder and Biliary Tract Malignancies
 Hepatic Malignancies and FDG PET/CT
Hepatic Malignancies and FDG PET/CT




Related posts:
Management of Hepatobiliary and Pancreatic Malignancies
Hepatobiliary and Pancreatic Malignancies: Epidemiology, Clinical Presentation, Diagnosis, and Staging
PET/CT in Pancreatic Malignancies
Pathology of Hepatobiliary and Pancreatic Cancer
PET/CT in Gall Bladder and Biliary Tract Malignancies
Hepatic Malignancies and FDG PET/CT
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
