- •
Radionuclide imaging artifacts are common and can lead to false positive results, decreasing the accuracy of the study.
- •
SPECT and PET imaging artifacts are related to equipment failure, reconstruction or postprocessing errors, or patient-related factors.
- •
Technologists and interpreting physicians must be aware of potential sources of artifact, how to detect and troubleshoot them, and, most importantly, how to prevent them from happening.
- •
The most common artifacts on SPECT imaging are patient-related and include motion and soft tissue attenuation.
- •
Prevention of patient motion in SPECT imaging requires attention to patient comfort on the imaging table and a thorough explanation of the procedure to improve patient cooperation. Attenuation artifacts can be overcome by repeating imaging in different position (e.g., prone, upright, or supine depending on equipment) or by having access to attenuation-correction hardware/software.
- •
The most common artifacts on PET imaging are related to patient motion and attenuation-correction errors primarily because of misalignment between the PET and the transmission scan. This is more common with PET/CT than with dedicated PET cameras.
- •
Prevention of patient motion in PET imaging requires similar strategies to those described for SPECT. Detection of misregistration or postprocessing artifacts with PET require careful review of the data. Most of these artifacts can be resolved using specialized software.
Introduction
Artifacts are a common source of error in single photon emission computed tomography (SPECT) and positron emission tomography (PET) imaging and can lead to false-positive results, decreasing the accuracy of the study and increasing the rates of unnecessary referral to coronary angiography. It is critical for clinicians and technologists to understand the mechanisms behind artifacts, methods to prevent and recognize artifacts, and solutions for correction. Artifacts may be related to sex, body habitus, soft tissue attenuation, body position under the camera, the type of imaging (SPECT or PET), or the choice of radiotracer. Many artifacts can be avoided by following standardized imaging protocols, and the majority can be identified and corrected in a timely fashion by nuclear technologists ( Table 5.1 ). Repeat imaging may be required for some artifacts, which adversely affects laboratory throughput and patient satisfaction (see Table 5.1 ). This chapter provides an overview of how to recognize, resolve, and prevent the typical SPECT and PET artifacts seen in routine practice.
| Artifact | Diagnosis | Prevention | |
| Patient-related | Attenuation | -Suspect when defects in locations known to be influenced by soft tissue attenuation. -Defects not conforming to typical coronary distribution. | -Comparable arm position between rest and stress images. -Routine use of attenuation correction techniques. |
| Breathing | Misregistration or blurry images. | -Counseling patient for shallow, slow, free breathing. | |
| Motion | Blurry images, opposite wall defects, abnormal LV cavity shape, motion on dynamic images. | -Counseling patient to lie as still as possible. -Assess for motion during image processing and use of motion correction algorithms. | |
| GI activity | -Review of images for some diaphragmatic activities, check contours and alignment. | -Keep patient NPO for 4 hours before study. -Use of adjunctive exercise. | |
| Obesity/count density | Poor image quality. | Image larger patients earlier in the generator life. | |
| Physiologic artifacts | May see persistent blood pool. | Longer prescan delay or may need to reprocess to only include later frames. | |
| Inadequate preparation | Myocardial flow reserve blunted at ~1.0. | Counseling patient on caffeine restriction, review of medications. | |
| Instrument related | Misregistration | Misalignment of PET emission and CT transmission data. | -Counseling patient on motion. -Careful review of alignment. -May need second CT transmission image after stress. |
| Beam hardening/metal | Focal/bright spots in known areas of hardware. | Check NAC images to see if the “bright spots” are artifact. | |
| Gating | Review of volume curves. | Data can be reprocessed to remove frames with significant ectopy. | |
| Attenuation correction | Focal/bright spots on AC images, but not noted on NAC images. | Review of both before meals and NAC images. | |
| Detector | Dark lines or streaks noted through the perfusion slices. | Regular quality assessment and assurance of camera integrity. | |
| Infusion system issue | Careful review of time/activity curves on dynamic images. | -Coordinated timing between technologist and camera imaging. -Checking for errors on the infusion system. |
SPECT imaging
Patient-related artifacts
Patient motion
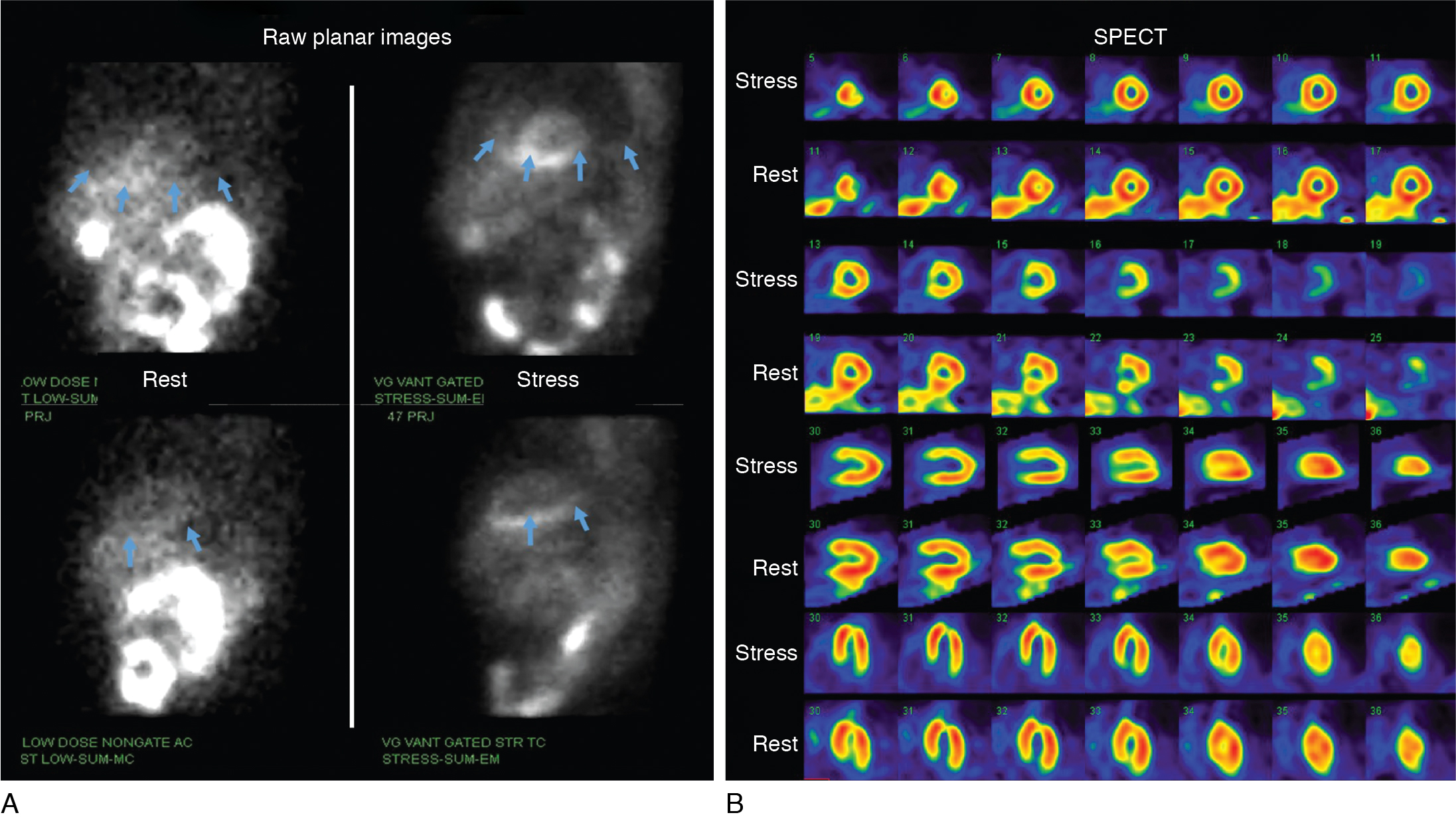
Motion is a common source of artifact in SPECT studies and can occur from patient motion while being imaged, respiratory motion, or cardiac creep. Frank patient motion can occur in the axial, lateral, or rotational direction. , Typically, motion in the axial direction or motion equal to or greater than one pixel is of greater consequence. Additionally, motion during the middle of the acquisition and abrupt motions are more likely to produce significant artifacts than gradual patient motion. Planar raw data, sinograms, and summed images of the planar projections should be carefully reviewed by both the technologist and interpreting physician. Imaging findings include defects on opposite walls, tails of diminished activity, or the so-called hurricane sign. Misalignment of left ventricular segments is also commonly seen, producing a tuning fork artifact ( Fig. 5.1 A–B–C). Cardiac creep consists of a gradual upward motion of the heart in the chest and can be seen when stress images are performed too soon after exercise. Early after exercise, the maximally expanded lung volume shifts the diaphragm and the heart downward at the start of the acquisition, which gradually moves up in the chest as the patient recovers from exercise and the lung volume returns to normal. Much of this can be prevented by waiting at least 15 minutes after an exercise stress test; by counseling the patient before imaging to lie still, not cough, and not fall asleep; and by ensuring the patient’s comfort and shortening imaging times as much as possible. Given that 99m technetium ( 99m Tc) has largely replaced 201 thallium ( 201 Tl) for SPECT myocardial perfusion imaging (MPI), this artifact is now seldom seen because of the typical longer delay from injection to acquisition of 99m Tc images (15 to 45 minutes) as described in Chapter 4 . Patient comfort should be ensured by carefully placing arms overhead to limit arm motion during image acquisition. Images should be evaluated carefully after each acquisition to assess for motion. Motion correction algorithms are now available in most commercially available SPECT processing software. , Although motion correction may reduce artifact severity, image quality may be adversely affected because of a lower count statistics secondary to removal of counts for motion correction (see Fig. 5.1 D). If motion correction does not substantially improve the artifact, images may have to be reacquired.


Attenuation artifacts
Photon attenuation by soft tissue is probably the most common source of artifacts seen on SPECT MPI. Degradation in image quality resulting from exaggerated soft tissue attenuation poses significant diagnostic challenges and is usually magnified in selected populations (e.g., obese people, women). Careful evaluation of rotating planar projection images should be performed for every study to identify potential sources of regional attenuation artifacts. One clue to the diagnosis of attenuation artifacts is that they may not conform to a particular coronary artery distribution. Although attenuation artifacts can affect any myocardial wall, those affecting the anterior or inferior wall are most common. The close proximity to the SPECT detector makes the lateral wall less vulnerable. Nevertheless, it can also be affected if the patient is imaged with the left arm down by the patient side. Computed tomography (CT) or radioactive line source-based attenuation correction can help minimize attenuation artifacts and false-positive findings.
Anterior wall
Breast or other chest wall soft tissue can significantly attenuate photons from the anterior wall in particular but also the lateral and inferior wall, causing artificially reduced counts in those areas. Although more prevalent in women, this type of artifact can also occur in men. If the breast position is consistent on both the stress and rest images, it will cause a similar decrease in counts on both imaging data sets. Normal wall motion and thickening in that area help confirm that the defect is likely secondary to attenuation and not a fixed perfusion defect from a prior infarct. This can be particularly problematic, however, if the breast shadow shifts position between stress and rest imaging. If the attenuation artifact only affects the stress images, it may show as a pseudoreversible defect that can result in a false-positive finding (the so-called shifting breast artifact, Fig. 5.2 ). Images should be carefully reviewed for the size and placement of the breast shadow and to see if any shift may have occurred between rest and stress. The technologists should ensure that the arms are placed above the head in similar positions between rest and stress so that the natural position of the breast will be similar in the two sets of images. Imaging without a bra is most helpful to minimize breast thickness or shifting breast artifacts.
Inferior wall
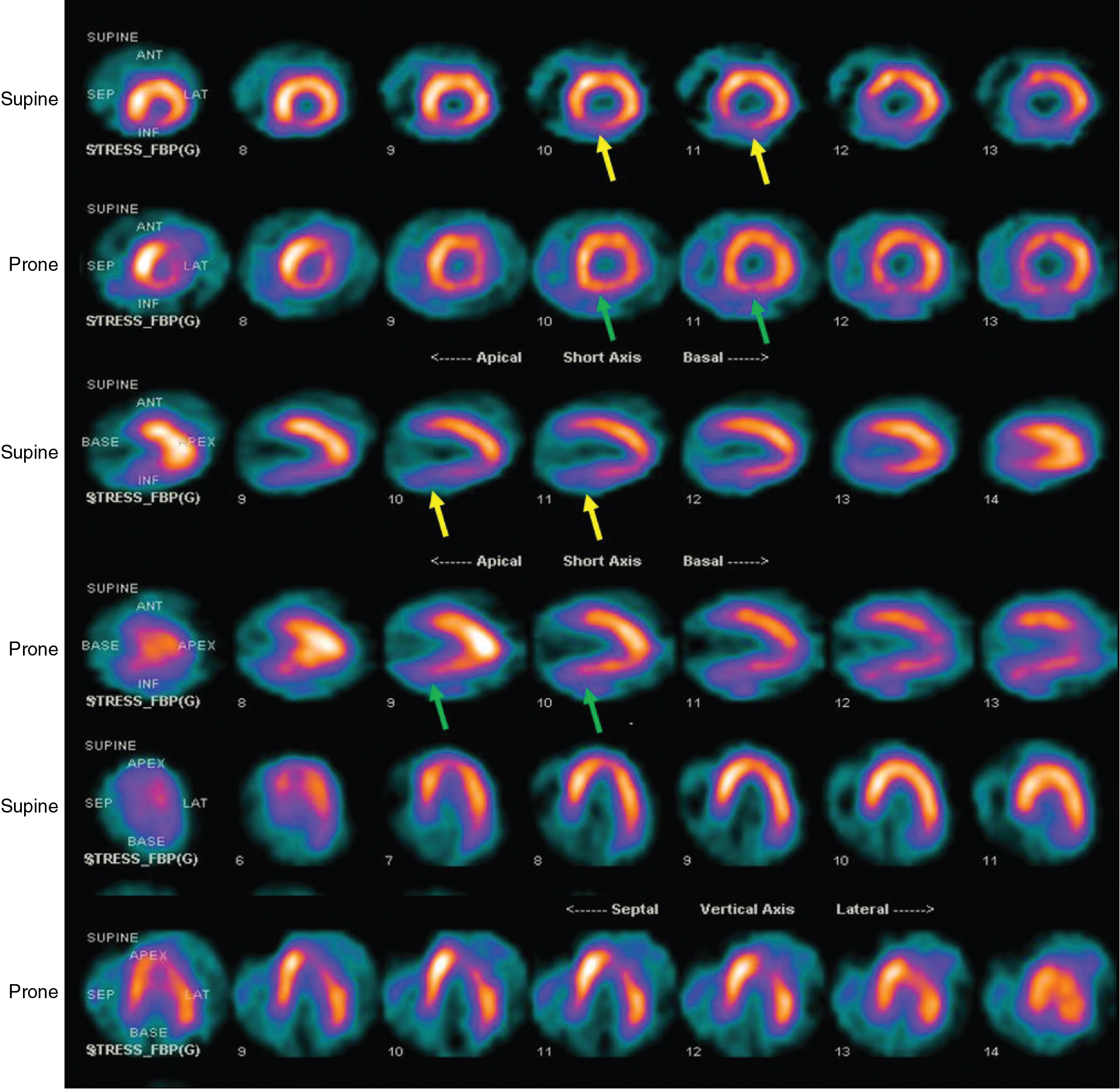
The left hemi-diaphragm may cause attenuation with decreased counts in the inferior or inferolateral walls and, in particular, in the basal inferior segment. This is most prevalent in obese patients who have an elevated left hemi-diaphragm; ascites; men; or when 201 Tl is used. Additionally, men have greater inferior attenuation compared with women. As previously discussed, careful attention to the raw images for the position of the diaphragm, along with assessment of wall motion and thickening in that area, helps to discern if the defect represents an attenuation artifact. In addition to attenuation correction, the use of prone imaging is quite helpful to reduce diagnostic uncertainty from inferior attenuation artifacts, especially when performing stress-first imaging protocols ( Fig. 5.3 ). Prone-only imaging has been evaluated as a diagnostic option, and although it may be more comfortable for some patients, a change in position can result in a change in attenuation from surrounding soft tissue, which has to be considered during image interpretation. It is for this reason that prone imaging is seldom used alone and two-position imaging is recommended to troubleshoot inferior attenuation artifacts.
Increased extracardiac activity
Subdiaphragmatic gastrointestinal (GI) radiotracer activity can significantly affect interpretation of the images and can either increase or decrease counts in the inferior wall of the heart. Significant GI activity immediately adjacent to the heart may cause scatter of photons, which may be misregistered as activity in the inferior left ventricular (LV) wall. This may mask ischemic defects on stress imaging. The additional counts scattered into the inferior wall may now be referenced as “normal,” and the normalization of the remaining myocardial counts to these segments may cause artifactual defects in the anterior or lateral walls. In addition, the contours generated by the processing software to delineate the LV boundaries may now include this adjacent GI activity, which will introduce errors into the calculation of LV function. Additionally, excessive isotope uptake in the liver can induce a ramp filter artifact (discussed later) and produce an inferior wall perfusion defect.
Strategies to reduce artifacts and improve recognition
Awareness of the potential patient-related causes of imaging artifacts is paramount to maximizing the value of radionuclide perfusion imaging. Patients who can exercise should preferentially undergo an exercise rather than pharmacologic stress test. An exercise stress test provides incremental diagnostic and prognostic value and also reduces liver and GI radioisotope uptake. This is because of the increased blood flow to the extremities during exercise and shunting of the blood away from the splanchnic circulation, thereby reducing liver and GI radioactivity. Additionally, among patients referred for vasodilator stress testing, a combination of low-level exercise and pharmacologic stress may also reduce subdiaphragmatic uptake and improve image quality ( Fig. 5.4 ). Having the patient drink a large amount of water to distend the stomach may also displace the bowel away from the heart and improve image quality on repeat acquisition. When increased liver uptake is noted, imaging should be repeated after a 30- to 45-minute delay to allow for the tracer activity to clear from the liver. The use of 99m Tc-labeled tracers also helps improve image quality and reduce attenuation artifacts.

 Careful attention should be paid to patient comfort, arm positioning, and counseling on laying still under the camera before beginning image acquisition. It is imperative to position the patient’s arms above the head consistently during rest and stress imaging. Careful review of the planar rotating images is critical to assess for any notable or moving soft tissue attenuation patterns between rest and stress, patient motion, and extracardiac activity that may lead to artifacts and false-positive studies ( Fig. 5.5 , ). Although Anger cameras with supine imaging are still the most prevalent SPECT systems, certain cameras allow for upright imaging as well (see Chapter 1 ). Upright imaging significantly improves patient comfort, thereby reducing motion artifacts and reducing the potential for shifting breast artifacts.
Careful attention should be paid to patient comfort, arm positioning, and counseling on laying still under the camera before beginning image acquisition. It is imperative to position the patient’s arms above the head consistently during rest and stress imaging. Careful review of the planar rotating images is critical to assess for any notable or moving soft tissue attenuation patterns between rest and stress, patient motion, and extracardiac activity that may lead to artifacts and false-positive studies ( Fig. 5.5 , ). Although Anger cameras with supine imaging are still the most prevalent SPECT systems, certain cameras allow for upright imaging as well (see Chapter 1 ). Upright imaging significantly improves patient comfort, thereby reducing motion artifacts and reducing the potential for shifting breast artifacts.

Soft tissue attenuation can be minimized by employing attenuation correction by means of a 153 gadolinium line source or CT in hybrid SPECT/CT systems. Unfortunately, attenuation-correction images can have their own range of artifacts and need to be reviewed carefully. In particular, transmission/emission misalignment, truncation artifacts, exaggerated apical thinning, and normalization issues are prevalent. , If attenuation-correction software is not available, repeat imaging with a change in patient position may need to be employed. For example, this may involve the addition of prone imaging to troubleshoot inferior defects as previously discussed (see Fig. 5.3 ).
Assessment of wall motion and thickening is critical for differentiating between infarction and attenuation artifacts in areas with fixed defects. The presence of normal regional wall motion and thickening in an area with a fixed defect is consistent with an attenuation artifact as opposed to prior myocardial infarction, especially in a patient without a history of prior coronary artery disease (CAD). Importantly, the presence of normal regional wall motion and thickening cannot be used to troubleshoot defects that show apparent reversibility.
Instrumentation-related artifacts
Hardware
Center of rotation artifact
Center of rotation is critically important, and cameras should be checked weekly for correct center of rotation alignment. This allows for the data from SPECT images that are processed with filtered backprojection to be aligned correctly. An error in the center of rotation by just a few pixels can result in blurring of images and produce artifactual defects on SPECT images.
Camera head misalignment
If the camera heads are misaligned, this can simulate center of rotation artifacts. Filtered backprojection of these misaligned images can cause artifactual imaging defects. These defects will be more pronounced with a triple-headed SPECT camera.
Nonuniformity
Uniformity of the flood fields is an extremely important quality assurance measure. This is to be performed with intrinsic flood fields on a daily basis and extrinsic flood fields weekly. Nonuniform distribution may occur secondary to defects in the photo multiplier tubes, collimator, or crystal or because of faulty electronics. Ring artifacts are produced in the transaxial slices and may artifactually appear as ischemic defects. When such artifacts are present, imaging should not be performed on the camera until uniformity is corrected.
Software
Ramp filter artifact
With traditional gamma cameras, a ramp filter is used to eliminate the star artifact in filtered backprojection reconstruction. When this is applied to areas with very intense activity along the inferior wall, in particular with GI or liver activity (left lobe of the liver), this can artificially decrease counts in the inferior wall, producing a prominent perfusion defect. This defect is referred to as a ramp filter artifact ( Fig. 5.6 ). Use of adjunctive low-level exercise with vasodilator stress reduces GI and liver activity and can thus reduce potential ramp filter artifacts. With the use of new SPECT systems employing iterative reconstruction over filtered backprojection, this artifact is becoming less common.