, Joungho Han2, Man Pyo Chung3 and Yeon Joo Jeong4
(1)
Department of Radiology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(2)
Department of Pathology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(3)
Department of Medicine Division of Pulmonary and Critical Care Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(4)
Department of Radiology, Pusan National University Hospital, Busan, Korea, Republic of (South Korea)
Abstract
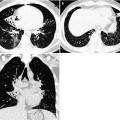
Reversed halo sign, which was named originally from the disease cryptogenic organizing pneumonia, refers to a focal, rounded area of ground-glass opacity surrounded by a more or less complete ring of consolidation [1, 2] (Fig. 8.1).
Definition
Reversed halo sign, which was named originally from the disease cryptogenic organizing pneumonia, refers to a focal, rounded area of ground-glass opacity surrounded by a more or less complete ring of consolidation [1, 2] (Fig. 8.1).
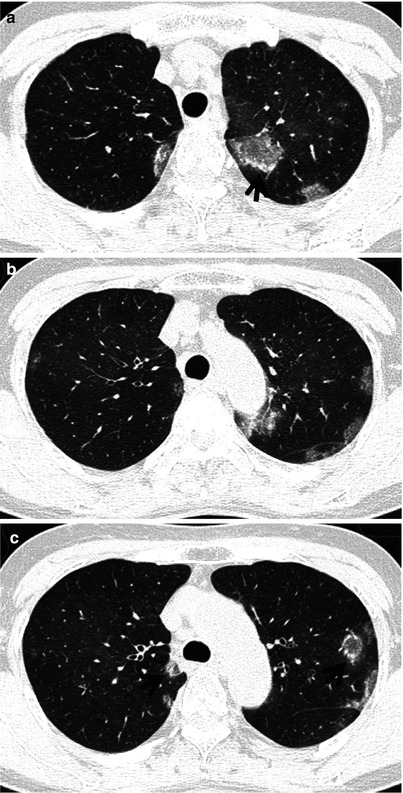
Fig. 8.1
Reversed halo sign in a 55-year-old asthmatic woman and chronic eosinophilic pneumonia. (a–c) Lung window images of thin-section (1.5-mm section thickness) scans obtained at levels of the great vessels (a), aortic arch (b), and azygos arch (c), respectively, show multifocal areas of ground-glass opacity in both lungs. Please note reversed halo sign (ground-glass opacity surrounded by a more or less complete ring of consolidation) (arrows) in both upper lobes
Diseases Causing the Sign
The reversed halo sign was first described as being relatively specific for cryptogenic organizing pneumonia (COP) (Fig. 8.2) or COP-like reaction but was later observed in several other infectious and noninfectious diseases. Pulmonary mucormycosis (former pulmonary zygomycosis) (Fig. 8.3) and invasive pulmonary aspergillosis may manifest the reversed halo sign [3]. Other causes of the reversed halo sign include noninvasive fungal infections such as paracoccidioidomycosis, histoplasmosis, and Pneumocystis jirovecii pneumonia [4]. Furthermore, pulmonary infarction [5], antineutrophil cytoplasmic antibody-associated granulomatous vasculitis (former Wegener’s granulomatosis), radiofrequency ablation, and lymphomatoid granulomatosis (Fig. 8.4) may also lead to this finding [6, 7] (Table 8.1).
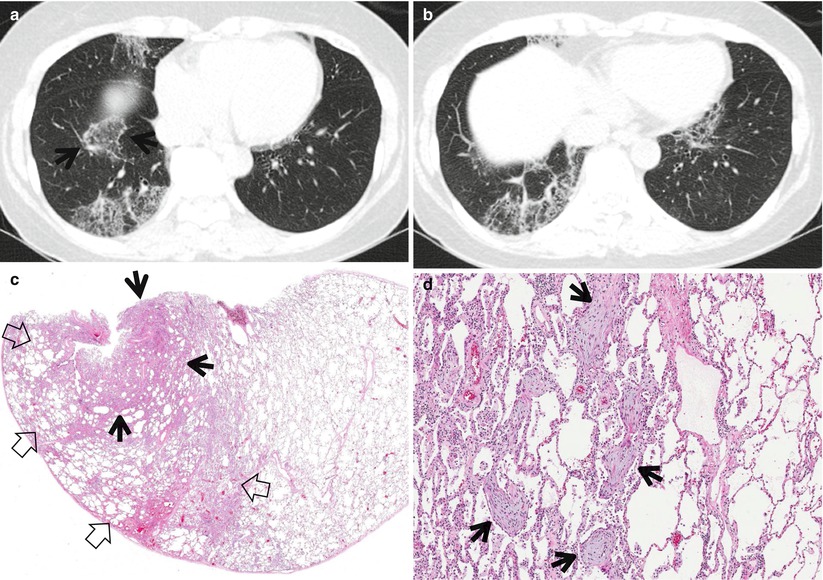
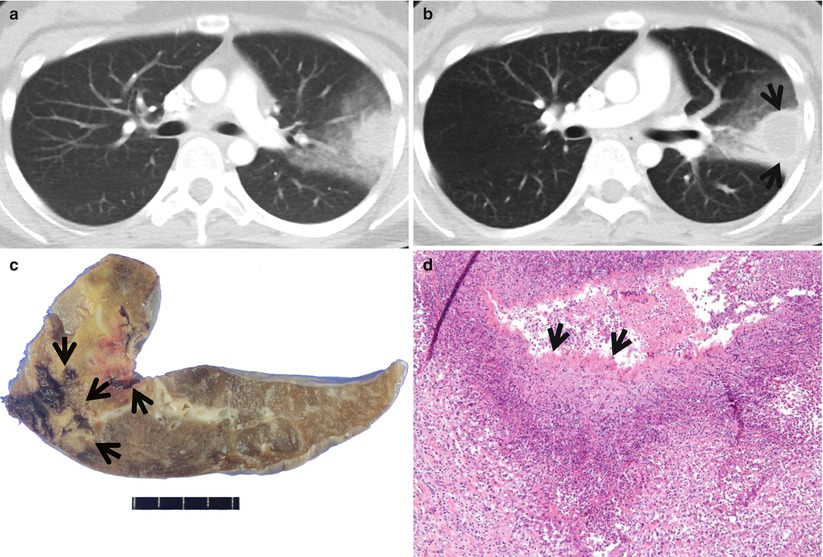

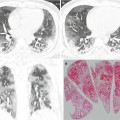
Fig. 8.2
Cryptogenic organizing pneumonia showing reversed halo sign in a 58-year-old woman. (a, b) Lung window images of thin-section (2.5-mm section thickness) scans obtained at levels of the suprahepatic inferior vena cava (a) and liver dome (b), respectively, show multifocal areas of ground-glass opacity in both lungs. Also note reversed halo sign area (arrows). (c) Low-magnification (×8) photomicrograph demonstrates somewhat denser area of consolidative area (arrows) and less dense area (open arrows) of interstitial inflammatory cell infiltration areas. Combination of these denser and less dense areas helps form reversed halo sign. (d) High-magnification (×100) photomicrograph discloses polyps (arrows) of fibroblast tissue within lumens of respiratory bronchioles, alveolar ducts, and alveoli. The interstitium is moderately thickened by mononuclear inflammatory cell infiltrates
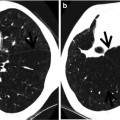
Fig. 8.3
Pulmonary mucormycosis in a 17-year-old woman who had a history of anaplastic large cell lymphoma 5 years ago. (a, b) Lung window images of enhanced consecutive CT scans (5.0-mm section thickness) obtained at levels of the right bronchus intermedius show dense consolidation surrounded by ground-glass opacity (a kind of halo sign). Please note internal reversed halo sign (arrows) formed by central necrosis and peripheral enhancing ring of consolidation. (c) Cut surface of gross specimen obtained with wide wedge resection of the left upper lobe by using video-assisted thoracoscopic surgery demonstrates invasive fungal consolidative lesion harboring necrotic cavity (arrows). (d) High-magnification photomicrograph (×100) discloses necrotizing pneumonia. Please note fungal organisms that have broad hyphae (arrows), thin wall, and little (pauci) septa
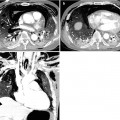
Fig. 8.4
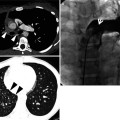
Lymphomatoid granulomatosis in a 70-year-old man showing reversed halo sign. Lung window image of CT scan (5.0-mm section thickness) obtained at level of the left lower lobar bronchus shows multiple variable-sized nodules in both lungs. Please also note bilaterally enlarged hilar lymph nodes. Some nodules show reversed halo sign (arrows)
Table 8.1
Common diseases manifesting as reversed halo sign
Disease | Key points for differential diagnosis |
|---|---|
Cryptogenic organizing pneumonia | Reversed halo sign, unilateral and bilateral consolidation with peribronchovascular and subpleural distribution |
Infectious disease | |
Mucormycosis | Reversed and CT halo sign |
Invasive pulmonary aspergillosis | Reversed and CT halo sign |
Paracoccidioidomycosis, histoplasmosis | |
Pulmonary infarction | Subpleural location |
ANCA-associated granulomatous vasculitis | Multiple, bilateral, subpleural nodules or masses |
Radiofrequency ablation | |
Lymphomatoid granulomatosis | Nodules and masses with central low attenuation and peripheral rim enhancement, CT halo or reversed halo sign |
Distribution
The reversed halo sign in COP may have its distribution along the subpleural lungs or the bronchovascular bundles [1]. In invasive fungal infection in immunocompromised patients, the sign appears as a large single lesion. In noninvasive fungal infection, the reversed halo sign(s) is usually associated with ground-glass opacity, small centrilobular nodules, or areas of consolidation, and the lesions are usually bilateral and asymmetric [4]. The reversed halo sign in chronic eosinophilic pneumonia may show upper and mid lung zone predominance, whereas pulmonary infarction may show subpleural location in pulmonary infarction.
Clinical Considerations
In neutropenic patients, the presence of reversed halo sign may suggest invasive fungal infection. Approximately 40 % of patients with chronic eosinophilic pneumonia have asthma; thus, reversed halo sign in asthmatics may imply chronic eosinophilic pneumonia [8]. In the situation of clinically pulmonary embolic disease, the presence of reversed halo sign hints the diagnosis of pulmonary infarction.
Key Points for Differential Diagnosis
1.




On CT scans, the reversed halo sign is observed in approximately 20 % of COP patients [1].
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
