Chapter 1
Right Upper Quadrant Pain
Charlotte Henningsen and Gregory Logsdon
• Describe the sonographic appearance of common gallbladder disease.
• List the risk factors associated with gallbladder disease.
• Identify laboratory values specific to gallbladder disease.
• Describe the sonographic appearance of liver cysts and abscesses.
• List the most common causes of abscess development in the liver.
• Describe the sonographic appearance of hematomas of the liver.
CLINICAL SCENARIO
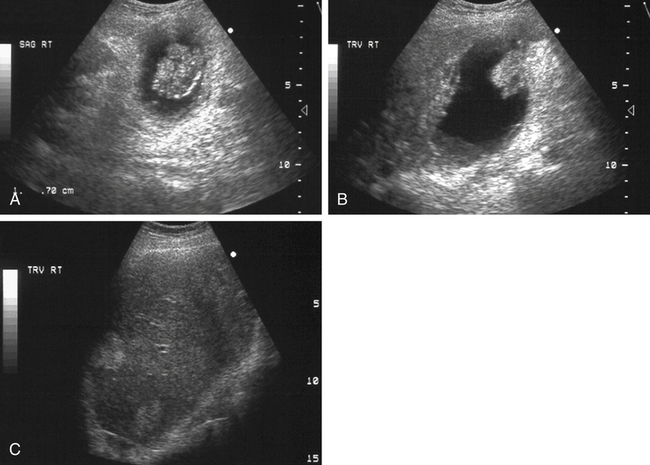
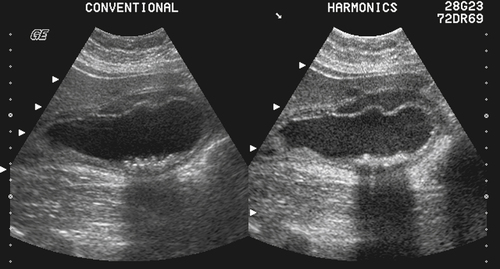
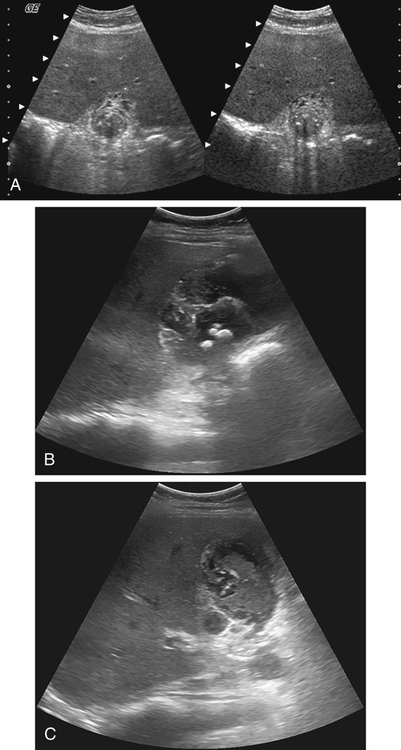
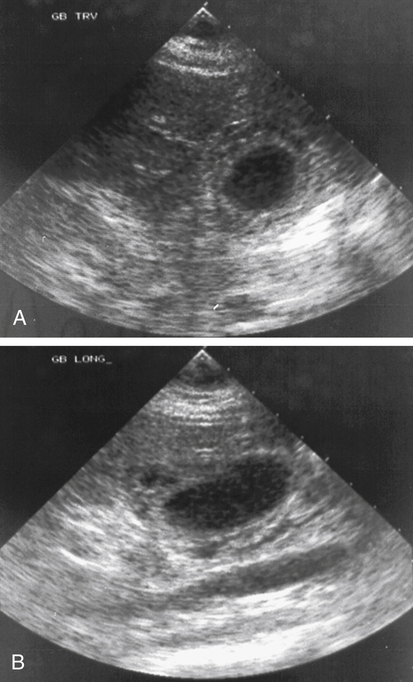
A 72-year-old man with right upper quadrant (RUQ) pain, nausea and vomiting, and unexplained weight loss is seen by his physician. The patient has a positive Murphy’s sign on clinical examination, and an RUQ ultrasound is ordered. The sonographic examination results reveal a thick-walled gallbladder with a 3.5-cm cauliflower-shaped mass projecting into the gallbladder in the fundal region (Fig. 1-1, A and B). A layering of low-level echoes also is identified in the dependent portion of the gallbladder that moves slowly with a change in patient position. The common bile duct (CBD) measures 4 mm. The sonographer also identifies two hyperechoic lesions in the liver (Fig. 1-1, C). What is the most likely diagnosis for this patient?
Right upper quadrant (RUQ) pain is a common clinical problem. The causes of RUQ pain include cholelithiasis and other gallbladder diseases; however, liver diseases and neoplasms (see Chapters 2 and 3) may manifest with similar symptoms. A thorough clinical examination, laboratory tests, and an RUQ ultrasound may be used to reveal the source of the discomfort. When gallbladder and liver diseases are suspected, the sonographer should take note of specific laboratory findings including bilirubin levels, liver function test results, and white blood cell counts.
In addition to the conditions discussed in this chapter, right-sided pain may be associated with diseases of the kidney (see Chapters 5, 6, and 7), the pancreas (see Chapter 4), and the gastrointestinal (GI) tract.
Gallbladder
Normal Sonographic Anatomy
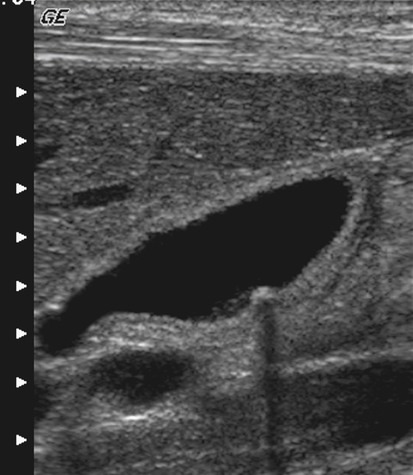
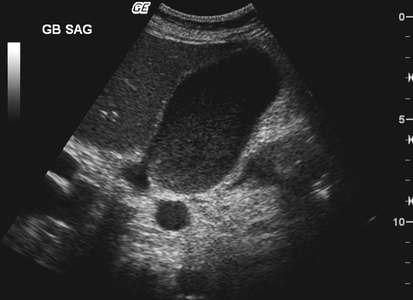
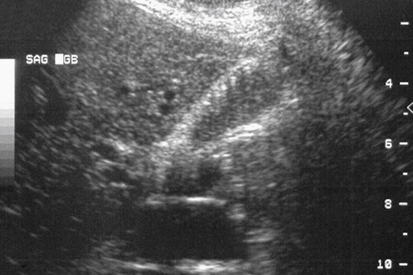
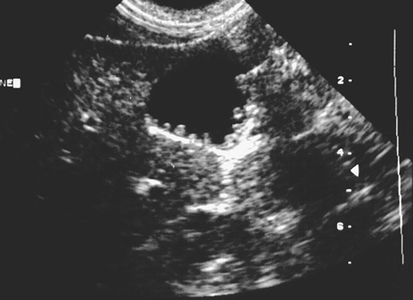
The gallbladder is a teardrop-shaped structure that is responsible for the concentration and storage of bile. The normal gallbladder is 7 to 10 cm in length and 2.5 to 4 cm in diameter. The lumen of the gallbladder is anechoic in normal circumstances, and the gallbladder wall appears thin and smooth, with a measurement of less than 3 mm in thickness (Fig. 1-2).1 A sonographic evaluation of the gallbladder should also include an evaluation of the bile ducts. The common bile duct (CBD) (Fig. 1-3) should measure 6 mm or less, and the common hepatic duct should measure 4 mm or less. The CBD size may be increased in patients who have undergone a cholecystectomy and in older patients.


Cholelithiasis
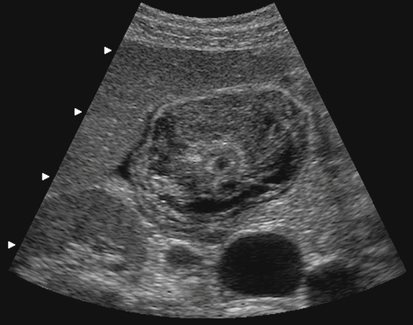
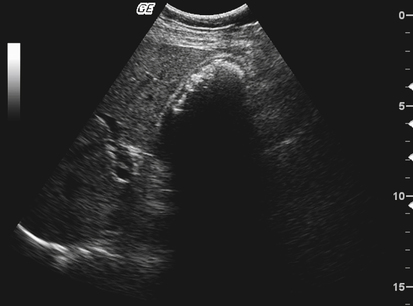
Cholelithiasis, also known as gallstones, is the most common disease of the gallbladder. Gallstones are usually composed of cholesterol, although stones may be made up of pigment or have a mixed composition. A predisposition for gallstone formation is seen in patients with impaired gallbladder motility and bile stasis. The typical patient has the “five f’s”: fat, female, forty, fertile, and flatulent. Family history, sedentary lifestyle, absence of alcohol use, and inflammatory bowel disease may contribute to gallstone formation; patients with gallstones also show an increased prevalence of heart disease.2 Other risk factors that predispose a patient to the development of gallstones include diet-induced weight loss, pregnancy (Fig. 1-4), total parenteral nutrition (TPN), diabetes, estrogen use, oral contraceptive use, hemolytic diseases, and white or Hispanic race. Cholelithiasis has also been identified in both genders, in children, and in the fetus.

Sludge
Sonographic Findings
The sonographic appearance of sludge is that of low- to medium-level echoes within the gallbladder (Fig. 1-6) that are nonshadowing, layer, and move slowly with a change in patient position from the viscous nature. Sludge may be identified in conjunction with cholelithiasis, cholecystitis, and other biliary diseases, including gallbladder carcinoma.
Cholecystitis
Acute Cholecystitis
The most common cause of acute cholecystitis is cholelithiasis that creates a cystic duct obstruction. Because of the high prevalence of associated cholelithiasis, acute cholecystitis is more common in female patients; however, when cholecystitis develops in male patients, it is usually more severe.3 Clinical symptoms include RUQ pain, fever, and leukocytosis. Serious complications can occur in patients with acute cholecystitis, including empyema, gangrenous cholecystitis, emphysematous cholecystitis, and gallbladder rupture.
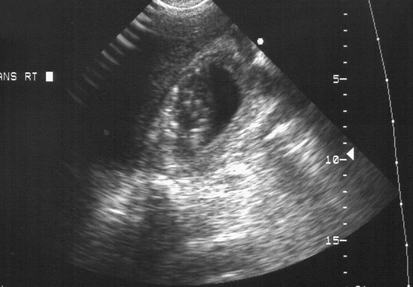
Acalculous cholecystitis (ACC) is an acute inflammation of the gallbladder in the absence of cholelithiasis (Fig. 1-7). The etiology is multifactorial. ACC occurs in patients with TPN, postoperative patients, and trauma and burn patients. ACC is more common in male patients.
Chronic Cholecystitis
Sonographic Findings
The sonographic findings suggestive of chronic cholecystitis include gallbladder wall thickening and cholelithiasis. The WES (wall, echo, shadow) sign is described as a contracted gallbladder and the presence of gallstones (Fig. 1-9) and may be identified in association with chronic cholecystitis, and cholelithiasis.
Emphysematous Cholecystitis
Emphysematous cholecystitis is a complication of acute cholecystitis in which gas invades the gallbladder wall and lumen, and may also be present in the biliary ducts. Emphysematous cholecystitis occurs with ischemia of the gallbladder wall and subsequent bacterial invasion. It is more common in male patients, and is frequently associated with underlying diseases such as diabetes mellitus and peripheral atherosclerotic disease.4 Complications of emphysematous cholecystitis include the development of gangrene of the gallbladder and gallbladder rupture.
Gangrenous Cholecystitis
Another complication of acute cholecystitis is gangrenous cholecystitis (Fig. 1-11), which is associated with increased morbidity and mortality and may lead to gallbladder perforation. The gallbladder wall is thickened and edematous, with focal areas of exudate, hemorrhage, and necrosis. Patients more commonly have generalized abdominal pain rather than a positive Murphy’s sign.
Sonographic Findings
The sonographic appearance of gangrenous cholecystitis includes focal thickening of the gallbladder wall, striations across the gallbladder wall (Fig. 1-12), intraluminal echoes, and intraluminal membranes. Pericholecystitic fluid may be present as well as cholelithiasis, which is often associated with gangrenous cholecystitis.
Gallbladder Perforation
Sonographic Findings
The sonographic findings of gallbladder perforation may include cholelithiasis, gallbladder wall thickening, intraluminal debris, and ascites. In addition, sonographic visualization of the gallbladder may reveal the actual perforation site in the gallbladder wall (described as the “hole” sign), pericholecystic abscess, and gallstones free-floating in ascites that surrounds the liver.5
Hyperplastic Cholecystosis
Adenomyomatosis
Adenomyomatosis of the gallbladder occurs with diffuse or localized hyperplasia of the gallbladder mucosa that extends into the muscular layer and results in mucosal diverticula, known as Rokitansky-Aschoff sinuses.6 Adenomyomatosis may be asymptomatic, or may be seen with symptoms similar to those of gallstones.
Sonographic Findings
Adenomyomatosis may appear sonographically as anechoic or echogenic foci within the gallbladder wall corresponding to the Rokitansky-Aschoff sinuses. Shadowing or comet-tail artifact (Fig. 1-13) may be seen emanating from the diverticula, and gallbladder wall thickening may be noted.7 Adenomyomatosis may also be seen in association with cholelithiasis.
Cholesterolosis
Sonographic Findings
Cholesterolosis may appear sonographically as multiple small cholesterol polyps that arise from the gallbladder wall (Fig. 1-14). These polypoid lesions do not shadow or move with variation in patient position. Comet-tail artifacts may also be identified emanating from the cholesterol polyps and may be indistinguishable sonographically from adenomyomatosis. Gallbladder polyps may also occur in isolation, and when they are small, they are insignificant.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


