Chapter 19 Sagittal magnetic resonance scans
Anyone who has undertaken the exercises described in Chapters 17 and 18, should find it straightforward to read sagittal, magnetic resonance image (MRI) scans of the lumbar spine. Those exercises asked the reader to expect the structures that lie anterior, lateral and posterior to the lumbar vertebral column. In plain radiographs, those structures were invisible, but in MRI scans, they are actually evident. Reading sagittal MRI scans, therefore, amounts to no more than matching expectation with what is actually evident.
1 Which parts of the vertebral column will be evident?
2 Which elements of the contents of the vertebral canal will be evident?
3 Which structures anterior to the vertebral column will be evident?
4 Which structures posterior to the vertebral column will be evident?
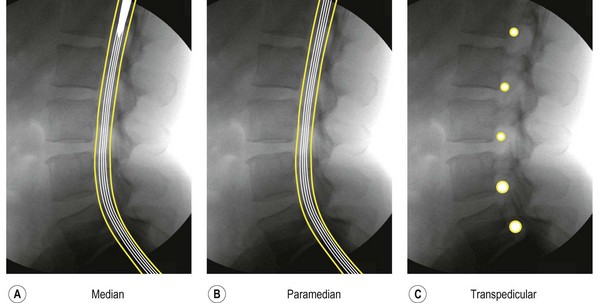
Sagittal MRI scans are typically taken across five standard planes (Fig. 19.1). Additional scans might be taken between these standard planes, or slightly displaced left or right from them; but the principles of analysis remain the same.
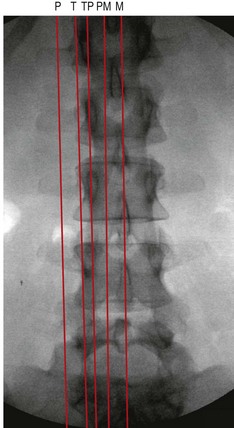
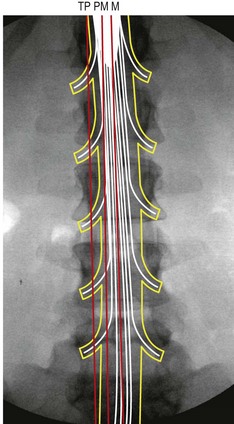
With respect to the contents of the vertebral canal, median, paramedian and transpedicular scans will intersect different components of the dural sac and its contents (Fig. 19.2). A median scan will intersect the conus medullaris of the spinal cord at upper segmental levels, and the cauda equina at lower levels. A paramedian scan may miss the spinal cord and show only the cauda equina. A transpedicular scan will intersect the spinal nerves and their dural sleeves, as they pass under the pedicles. Tangential and peripheral scans will not intersect the contents of the vertebral canal.
In a lateral view, the reader should, therefore, expect a median scan to show the dural sac, the conus medullaris of the spinal cord and the cauda equina (Fig. 19.3A). A paramedian scan would show only the cauda equina (Fig. 19.3B). A transpedicular scan would show only the spinal nerve roots and their sleeves (Fig. 19.3C).