SECTION VIII NEURORADIOLOGY IMAGING
Essentials 1
Case
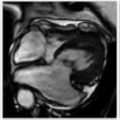
A 6-day-old term neonatal boy presents with an abnormal electroencephalogram following prolonged perinatal resuscitation.

Questions
1. What is the MOST likely diagnosis?
A. Metachromatic leukodystrophy
B. Severe global hypoxic-ischemic injury
C. Pantothenate kinase-associated neuropathy
D. Mitochondrial encephalopathy with lactic acidosis and stroke-like episodes
E. X-linked adrenoleukodystrophy
2. Which of the following structures is MOST commonly affected in a term neonate when this injury occurs in a partial prolonged manner?
A. Thalamus
B. Putamen
C. Watershed zones (border zones)
D. Cerebellum
E. Pons
3. What property of tissue in the central nervous system is responsible for differences in signal intensity on diffusion-weighted imaging?
A. Axonal cytoskeleton
B. Myelin sheaths
C. Fast-axonal transport systems
D. Intact cell membranes
E. Osmolality
Answers and Explanations
Question 1
B. Correct! This is hypoxic-ischemic injury (HII). Areas of active myelination are most susceptible to ischemic injury in the term neonate. As such, the basal ganglia (particularly the posterior putamina), ventrolateral thalami, hippocampus, dorsal brainstem, corticospinal tracts, and perirolandic regions are most affected by severe HII. In the acute phase, these areas will exhibit restricted diffusion, although normal findings have rarely been reported in the first 24 hours. In the preterm infant, severe HII affects the thalami and brainstem with relative preservation of the basal ganglia and cerebral cortex.
Other choices and discussion
A. Metachromatic leukodystrophy is a lysosomal storage disease that typically presents with symmetric and confluent T2 hyperintense signal in the periventricular white matter. This may have a “tiger-stripe” appearance due to areas of preserved myelination along medullary veins. Given the absence of these findings and the presence of symmetric restricted diffusion involving the basal ganglia, optic radiations, and perirolandic regions in the test case, metachromatic leukodystrophy is incorrect.
C. Pantothenate kinase-associated neuropathy is a type of neurodegeneration with brain iron accumulatio. It has an autosomal recessive inheritance pattern. The classic imaging finding is that of T2 hypointense signal in the globus pallidus with central hyperintensity (“eye of the tiger” sign), which is not present in this case.
D. Typical imaging findings in mitochondrial encephalopathy with lactic acidosis and stroke-like episodes are stroke-like lesions in the cortex that do not conform to a vascular territory. Parietal and occipital cortices are involved most frequently. Other findings include lacunar infarcts and basal ganglia calcifications. These findings are not shown in the test case. Symptoms of mitochondrial encephalopathy with lactic acidosis and stroke-like episodes do not tend to manifest until adolescence.
E. X-linked adrenoleukodystrophy is a peroxisomal disorder seen in male children. Imaging findings include T2 hyperintense signal beginning in the splenium of the corpus callosum and spreading peripherally as the disease progresses. Contrast enhancement is seen in the intermediate zone of the demyelinated area, along the periphery (“leading edge” enhancement). Primary involvement of the deep gray matter and cortices in the test case argues against X-linked adrenoleukodystrophy.
Question 2
C. Correct! During prolonged periods of partial asphyxia in the term neonate, blood is preferentially shunted to the deep gray matter, brainstem, and cerebellum at the expense of the white matter and cortex, resulting in injury to the cerebral watershed or border zones. In the preterm infant, less profound HII results in germinal matrix hemorrhage and deep periventricular white matter injury.
Other choices and discussion
A. The thalamus is generally spared in partial prolonged asphyxia but involved in severe HII. Severe HII in the term neonate also involves the basal ganglia (especially the posterior putamina), ventrolateral thalami, hippocampi, dorsal brainstem, corticospinal tracts, and perirolandic cortices. On the contrary, partial prolonged asphyxia in the term neonate typically affects the watershed areas in the brain.
B. The putamen is generally spared in partial prolonged asphyxia but involved in severe HII.
D. The cerebellum is spared.
E. The pons is spared.
Question 3
D. Correct! Diffusion-weighted imaging generates a map of the apparent diffusivity (measured by apparent diffusion coefficient) of water molecules in their microenvironment. The term “apparent” is used because while the true diffusivity of water is constant, its apparent diffusivity is influenced by its environment. In the brain, intact cell membranes hinder the diffusion of water molecules, giving the appearance that the diffusivity of water in the parenchyma is reduced relative to the diffusivity of water in cerebrospinal fluid. Various pathologies further reduce the apparent diffusivity of water (i.e., cause restricted diffusion, as reflected by bright diffusion-weighted imaging and dark apparent diffusion coefficient signal intensity) with respect to normal brain, including anything causing cytotoxic edema (e.g. infarction), hematomas at certain stages, purulent material (in abscesses), and tumors with high nucleus-to-cytoplasmic ratios.
The other choices are all incorrect.
Suggested Readings
Gillard JH, Waldman AD, Barker PB, eds. Clinical MR Neuroimaging: Diffusion, Perfusion, and Spectroscopy. Cambridge: Cambridge University Press; 2005 Huang BY, Castillo M. Hypoxic-ischemic brain injury: imaging findings from birth to adulthood. Radiographics 2008;28:417–439 Osborn AG. Osborn’s Brain: Imaging, Pathology, and Anatomy. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2012Top Tips
Severe HII in the term neonate involves the basal ganglia (posterior putamina), ventrolateral thalami, hippocampi, dorsal brainstem, corticospinal tracts, and perirolandic cortices.
Partial prolonged asphyxia in the term neonate often affects the cerebral watershed areas.
Look for symmetric restricted diffusion of the affected areas within 24 hours of the insult.
Essentials 2
Case
A 68-year-old man presents with confusion, unstable gait, and slurring of speech.

Questions
1. What is the MOST likely diagnosis?
A. Metastatic disease
B. Invasive fungal infection
C. Lymphoma
D. Multifocal glioblastoma
E. Subacute infarction
2. What is the approximate timeline and pattern of parenchymal enhancement after the injury from the test case occurs?
A. Enhancement begins at 2 hours, peaks at 2 days, and disappears by 2 weeks
B. Enhancement begins at 1 day, peaks at 1 week, and disappears by 1 month
C. Enhancement begins at 2 days, peaks at 2 weeks, and disappears by 2 months
D. Enhancement begins at 4 days, peaks at 4 weeks, and disappears by 4 months
E. Enhancement begins at 7 days, peaks at 4 weeks, and disappears by 4 months
3. What is the name for the finding of serpiginous cortical T1 hyperintensity that is often seen with subacute infarcts?
A. Cortical ribboning
B. Cortical laminar necrosis
C. Cortical tram-track sign
D. Cortical rim sign
E. Transmantle sign
Answers and Explanations
Question 1
E. Correct! This patient has a subacute infarction. The findings of cortical or gyral edema and contrast enhancement in the distribution of a vascular territory (middle cerebral artery territory in this patient) are most consistent with subacute infarction. Parenchymal enhancement is caused by leakage of the contrast agent across the disrupted blood–brain barrier. Enhancement can be gyral (if cortical involvement is present) or generalized or ring-like (if basal ganglia or brainstem involvement is present). It usually begins at the end of the first week following complete infarction and typically disappears by 2 months. However, parenchymal cortical enhancement can also be seen with incomplete infarction, usually occurring between 2 to 4 hours after the ischemia onset and disappearing 24 to 48 hours later. This type of enhancement is postulated to occur from vascular occlusion with very early reperfusion and is associated with a good prognosis. Of note, intravascular (arterial) and meningeal enhancement can be seen with acute infarcts, which are commonly seen and resolve within the first week of a stroke.
Discussion
The other choices are all incorrect. The gyral pattern of enhancement, lack of edema relative to the size of the enhancing lesions on fluid-attenuated inversion recovery imaging, and location of the lesions within a vascular (right middle cerebral artery) territory make metastatic disease, invasive fungal infection, lymphoma, and multifocal glioblastoma unlikely. Note that invasive fungal infections can sometimes cause infarct-like lesions.
Question 2
C. Correct! Enhancement begins at 2 days, peaks at 2 weeks, and disappears by 2 months. The “2-2-2 rule” is a good approximation of the timeline and pattern of parenchymal enhancement following an ischemic event. It typically begins 4 to 7 days after complete infarction but can be seen as early as 1 to 2 days after the event. In the majority of strokes, enhancement is present between 1 week and 2 months, although it can persist for up to 4 months. An alternative diagnosis should be considered if enhancement persists beyond this time. Of note, the presence of early parenchymal enhancement within 6 hours of a stroke predicts a higher risk for hemorrhagic transformation, especially if the stroke is located in the basal ganglia or deep gray matter.
The other choices are all incorrect.
Question 3
B. Correct! Cortical laminar necrosis, or pseudolaminar necrosis, is due to oxygen and/or glucose depletion and mainly affects the third layer of the cerebral cortex, which is the most vulnerable of the six cortical layers to hypoxia and hypoglycemia. The T1 hyperintensity is related to denatured proteins in necrotic cells or fat-laden macrophages, not from calcium or hemoglobin products. This phenomenon is often detected 2 weeks after a stroke and can be seen as early as 3 to 5 days following the event. It typically resolves after 3 months but may persist for more than a year.
Other choices and discussion
A. Cortical ribboning is hyperintensity of the cortex on diffusion-weighted imaging and is a useful diagnostic sign of Creutzfeldt-Jacob disease.
C. Cortical tram-track sign is produced by cortical calcifications due to leptomeningeal vascular anomalies in patients with Sturge-Weber syndrome.
D. Cortical rim sign is useful to distinguish renal infarct from acute pyelonephritis. It denotes continued enhancement of the peripheral cortex of an infarcted kidney because of capsular collateral arteries.
E. Transmantle sign is an imaging feature of focal cortical dysplasia. It is most often found in type 2 focal cortical dysplasia (Taylor-type dysplasia). This dysplasia is characterized by linear T2/fluid-attenuated inversion recovery signal extending from the ventricle to the cortex and represents arrested neuronal migration.
Suggested Readings
Allen LM, Hasso AN, Handwerker J, et al. Sequence-specific MR imaging findings that are useful in dating ischemic stroke. Radiographics 2012;32:1285–1297 Karonen JO, Partanen PL, Vanninen RL, et al. Evolution of MR contrast enhancement patterns during the first week after acute ischemic stroke. Am J Neuroradiol 2001;22:103–111 Seth NK, Torgovnick J, Macaluso C, et al. Cortical laminar necrosis following anoxic encephalopathy. Neurol India 2006;54:327Top Tips
Remember the “2-2-2” enhancement rule for subacute infarcts: enhancement begins at 2 days, peaks at 2 weeks, and disappears by 2 months.
Enhancement can be gyral or ring-like. Remember the mnemonic MAGIC DR for rim-enhancing brain lesions: metastases, abscess, glioblastoma, infarct (subacute), contusion, demyelinating diseases, radiation necrosis.
Cortical laminar necrosis (or pseudolaminar necrosis), characterized by gyral T1 hyperintensity, is usually seen 2 weeks after infarction but can occur as early as 3 to 5 days after a stroke.
Essentials 3
Case
A 50-year-old woman with a history of alcoholism presents with acute alcoholic hepatitis, septic shock, and somnolence.

Questions
1. What is the MOST likely diagnosis?
A. Abscess
B. Acute infarction
C. Osmotic demyelination syndrome
D. Posterior reversible encephalopathy syndrome
E. Glioma
2. The most frequent cause of this disorder is rapid correction of which ONE of the following?
A. Hyponatremia
B. Hypokalemia
C. Hypocalcemia
D. Hypophosphatemia
E. Hypomagnesemia
3. Which of the following comprises the clinical symptoms that can be seen from brainstem injury due to osmotic demyelination syndrome (central pontine myelinolysis)?
A. Quadriplegia, dysarthria, dysphagia, lethargy
B. Quadriplegia, dysarthria, dysphagia, tremor
C. Diplopia, dysarthria, dysphagia, tremor
D. Locked-in syndrome, dysarthria, dysphagia, tremor
E. Amnesia, dysarthria, dysphagia, tremor
Answers and Explanations
Question 1
C. Correct! This patient has osmotic demyelination syndrome (ODS). “Trident-shaped” T2 or T2/fluid-attenuated inversion recovery hyperintense signal sparing the corticospinal tracts and ventrolateral pons, as in the test case, is characteristic of pontine involvement by ODS. Restricted diffusion, which is also seen, indicates the acute phase of disease. While ODS most frequently involves the pons, extrapontine involvement—including the thalamus, basal ganglia, white matter, and rarely, the cerebral cortex—may also be seen.
Other choices and discussion
A. On magnetic resonance imaging, an abscess appears as a central core of T2 hyperintensity and restricted diffusion surrounded by a thin T2 hypointense and enhancing rim. In the above case, while the lesion itself demonstrates T2 hyperintensity and restricted diffusion, the absence of a thin T2 hypointense rim, mass effect, and edema makes this answer choice incorrect.
B. An acute pontine infarct would appear as a focal paramedian lesion exhibiting restricted diffusion. Pontine infarcts result from thrombosis of pontine perforators arising from the basilar artery. Central and symmetric restricted diffusion surrounding the corticospinal tracts in the test case makes pontine infarct unlikely.
D. The central variant of posterior reversible encephalopathy syndrome (PRES), which is an uncommon pattern of PRES, may involve the brainstem, cerebellum, thalamus, and basal ganglia. Pontine involvement may be patchy or diffuse, but sparing of the corticospinal tracts as seen in the test case would not be expected with PRES. The most typical appearance of PRES, occurring in > 90% of cases, is vasogenic edema within the parietal and occipital lobes.
E. The absence of mass effect and the sparing of the corticospinal tracts argue against the diagnosis of glioma.
Question 2
A. Correct! The most frequent cause of ODS is rapid correction of hyponatremia. To prevent ODS, hyponatremia should be corrected at a rate of no more than 8 to 12 mmol/L of sodium per day. The rate of rise in plasma sodium concentration should be even lower in patients at higher risk for osmotic demyelination, such as those with chronic alcoholism, cirrhosis, and malnutrition.
Other choices and discussion
B. While concomitant hypokalemia may play a contributory role, the pathogenesis of ODS is secondary to the rapid correction of hyponatremia.
C. Rapid correction of hypocalcemia can contribute to cardiac arrhythmias and is not associated with ODS.
D. Rapid correction of hypophosphatemia can lead to complications such as hypocalcemia, tetany, and hypotension.
E. Hypomagnesemia is incorrect.
Question 3
A. Correct! The clinical manifestations of ODS become apparent 2 to 6 days following the rapid correction of sodium. Symptoms/signs that can be seen with the pontine variant of ODS (central pontine myelinolysis) include anything neurologically related to brainstem injury such as quadriplegia, dysarthria, dysphagia, lethargy, diplopia, and locked-in syndrome. Locked-in syndrome is a condition in which the patient is conscious and awake but globally paralyzed except for the ability to move his or her eyes; this syndrome often results from an acute lesion involving the ventral pons.
Other choices and discussion
The other choices are all incorrect. Whereas quadriplegia, dysarthria, dysphagia, diplopia, and locked-in syndrome can be seen with central pontine myelinolysis due to brainstem involvement, tremor and other movement disorders are typically seen with the extrapontine variant of ODS (extrapontine myelinolysis) affecting the basal ganglia. In addition, amnesia is not usually associated with ODS.
Suggested Readings
Howard SA, Barletta JA, Klufas RA, et al. Best cases from AFIP: osmotic demyelination syndrome. Radiographics 2009;29:933–988 Huq S, Wong M, Chan H, et al. Osmotic demyelination syndromes: central and extrapontine myelinolysis. J Clin Neurosci 2007;14;684–688 King JD, Rosner MH. Osmotic demyelination syndrome. Am J Med Sci 2010;339:561–567Top Tips
ODS is most often the result of rapid chronic hyponatremia correction.
Common conditions associated with ODS: alcoholism, malnutrition, and liver transplantation.
Pontine involvement by acute ODS (“central pontine myelinolysis”) appears on magnetic resonance imaging as “trident-shaped” T2 hyperintensity and restricted diffusion in the central pons sparing the corticospinal tracts and ventrolateral pons.
Essentials 4
Case
A 55-year-old woman presents with history of rheumatoid arthritis presents with left complete hemianopsia.

Questions
1. What is the MOST likely diagnosis?
A. Metastasis
B. Pyogenic abscess
C. Tumefactive demyelinating lesion
D. Acute infarction
E. Hematoma
2. Which pattern of enhancement is MOST characteristic of this process?
A. Ring enhancement with enhancing nodule
B. Open ring or incomplete ring enhancement
C. Thick and irregular ring enhancement
D. Gyral enhancement
E. Nodular enhancement
3. Which of the following is an immune-mediated microvascular endothelial disorder characterized by the following clinical triad: encephalopathy, sensorineural hearing loss, and vision impairment?
A. Multiple sclerosis
B. Acute disseminated encephalomyelitis
C. Neuromyelitis optica
D. Progressive multifocal leukoencephalopathy
E. Susac syndrome
Answers and Explanations
Question 1
C. Correct! This is a tumefactive demyelinating lesion (TDL). TDLs are well circumscribed, exert little mass effect, and produce relatively little surrounding edema for their size. Enhancement is variable but, when present, appears as an incomplete ring of enhancement (“leading edge” enhancement), as in this case. Apparent diffusion coefficient values are elevated (facilitated diffusion) in the lesion as a whole, although peripheral restricted diffusion can be observed, a feature also present in the test case. While the natural progression of TDLs is unknown, a number of studies have reported that most patients with TDLs will be eventually diagnosed with multiple sclerosis (MS) or a neuromyelitis optica spectrum disorder. A subset of patients does not progress to typical MS. The majority of patients with TDLs respond favorably to corticosteroid therapy.
Other choices and discussion
A. The marked hyperintense T2 signal intensity, incomplete rim of restricted diffusion and enhancement, and relative paucity of perilesional edema in this case argues against metastatic disease.
B. The classic appearance of a mature pyogenic abscess is a round mass with a relatively T1 hyperintense and T2 hypointense rim, a complete rim of enhancement that may be thinner along the ventricular side, and a core of T2 hyperintense signal and restricted diffusion representing the walled-off purulent material. Mass effect and surrounding edema is common. In the above case, the lesion demonstrates restricted diffusion along the periphery, making this answer choice unlikely.
D. The test case does not conform to a vascular distribution and is confined to the white matter, making acute infarction unlikely.
E. The imaging appearance of a hematoma varies depending on the age of the hemorrhage. Although the solid clot component of a hematoma can exhibit restricted diffusion, the peripheral pattern of restricted diffusion (and marked T2 hyperintensity of the lesion), as seen in the test case, is not typical of hematoma.
Question 2
B. Correct! An open or incomplete ring of enhancement is most suggestive of a demyelinating process, although enhancement may be variable. The enhancing portion of the lesion is thought to represent the leading edge of demyelination.
Other choices and discussion
A. Ring enhancement with enhancing nodule is more typical of infectious or neoplastic processes. Toxoplasmosis, neurocysticercosis, metastases, and some primary brain tumors can have this appearance.
C. Thick and irregular ring enhancement is more suggestive of a necrotic neoplasm.
D. Gyral enhancement can be seen in the subacute phase of cerebral infarction following reperfusion.
E. Nodular enhancement can be seen in the setting of metastasis, septic emboli, and granulomatous processes.
Question 3
E. Correct! Susac syndrome (retinocochleocerebral vasculopathy) is an immune-mediated microvascular occlusive endotheliopathy. Patients present with the clinical triad of encephalopathy, sensorineural hearing loss, and vision impairment due to branch retinal artery occlusions. Magnetic resonance imaging shows multiple T2 hyperintense lesions in the brain, including the corpus callosum, that can mimic MS. In Susac syndrome, there is involvement of the middle layer of the corpus callosum with sparing of the undersurface, whereas in MS, the undersurface is involved.
Other choices and discussion
A. MS is the most common primary demyelinating disorder of the central nervous system involving the brain and spinal cord. Magnetic resonance imaging demonstrates multiple, usually small, T2 hyperintense plaques that characteristically involve the callososeptal interface with perivenular extension (“Dawson’s fingers”). Therefore, white matter spots in the brain that appear ovoid in shape and are oriented perpendicular to the plane of the lateral ventricles should raise the suspicion for underlying MS. The diagnosis of MS itself is based on both clinical and imaging findings, taking into account the Revised McDonald criteria, which characterizes lesions disseminated in space and time, and presence of oligoclonal immunoglobulin-G bands in cerebrospinal fluid.
B. Acute disseminated encephalomyelitis is an immune-mediated demyelinating disorder that can occur weeks following a viral prodrome or vaccination. In contrast to MS, acute disseminated encephalomyelitis is usually a monophasic illness and occurs most frequently in children.
C. Neuromyelitis optica, also known as Devic syndrome, is an immune-mediated demyelinating disease that preferentially involves the optic nerves (optic neuritis) and spinal cord (transverse myelitis).
D. Progressive multifocal leukoencephalopathy is an infectious demyelinating process caused by reactivation of the human polyomavirus JC in immunocompromised patients.
Suggested Readings
Dagher AP, Smirniotopoulos J. Tumefactive demyelinating lesions. Neuroradiology 1996;38:560–565Top Tips
TDLs are large (> 2 cm) lesions that usually involve the white matter and have little mass effect and edema for their size.
Open or incomplete ring enhancement and restricted diffusion along the periphery of a lesion are characteristic imaging features of demyelinating lesions.
Although many patients with TDLs will be eventually diagnosed with MS, a number of patients will not progress to MS.
Essentials 5
Case
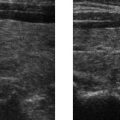
A 35-year-old woman with migraine history presents with acute onset headache differing in quality from her usual headaches. Magnetic resonance imaging of the brain (not shown) was normal. Magnetic resonance angiography was performed at presentation (left) and at 3-month follow up (right). Erythrocyte sedimentation rate and C-reactive protein levels were normal.

Questions
1. What is the MOST likely diagnosis?
A. Moyamoya disease
B. Dissection
C. Reversible cerebral vasoconstriction syndrome
D. Vasculitis
E. Atherosclerotic disease
2. What is the MOST common clinical presentation of this disorder?
A. Thunderclap headache
B. Seizure
C. Syncope
D. Sudden onset focal neurologic deficit
E. Encephalopathy
3. Most patients with reversible cerebral vasoconstriction syndrome have normal nonvascular brain imaging, although some may have positive findings such as hemorrhage, vasogenic edema, and infarction. These findings BEST overlap with which ONE of the following disorders?
A. Progressive multifocal leukoencephalopathy
B. Posterior circulation stroke
C. Venous sinus thrombosis
D. Gliomatosis cerebri
E. Posterior reversible encephalopathy syndrome
Answers and Explanations
Question 1
C. Correct! This is reversible cerebral vasoconstriction syndrome (RCVS), also known as Call-Fleming syndrome. RCVS is a clinical and radiographic syndrome manifested by hyperacute onset of severe headache with segmental cerebral arterial vasoconstriction that can affect the anterior and/or posterior circulation(s). The test case clinical presentation of a severe and sudden onset headache with self-limited angiographic findings of multifocal narrowing involving the superior cerebellar and posterior cerebral arteries is typical of RCVS. By definition, the vasoconstriction with RCVS should resolve within 3 months. It occurs most frequently in young to middle-aged adults, and women are more affected than men. While a third of cases may occur spontaneously, a specific trigger can be identified in some patients (e.g., complications of pregnancy such as eclampsia or preeclampsia, postpartum state, and exposure to vasoactive or recreational drugs such as cocaine, cannabis, ecstasy, selective serotonin reuptake inhibitors, nasal decongestants, pseudoephedrine, and migraine medications).
Other choices and discussion
A. Moyamoya disease is a progressive arteriopathy characterized by progressive stenosis of the supraclinoid internal carotid arteries. In Japanese, the name “moyamoya” means “puff of smoke” and describes the appearance of small collateral vessels that form to compensate for arterial occlusions. Involvement of the posterior circulation occurs less frequently, and when it does occur, anterior circulation steno-occlusive disease is also usually present. Unlike RCVS, imaging findings do not resolve on follow up imaging.
B. Dissection would not present as transient and self-limited multifocal narrowing of the bilateral posterior cerebral and superior cerebellar arteries.
D. Imaging findings of central nervous system vasculitis include multisegmental narrowing of the cerebral arteries, and while patients may also present with headache, the headache tends to be more subacute and insidious in onset than in this test case. In contrast to RCVS, imaging findings would not be expected to improve without appropriate treatment. In addition, serum markers of inflammation, such as erythrocyte sedimentation rate and C-reactive protein, are often elevated in patients with vasculitis and not elevated in patients with RCVS.
E. Atherosclerotic vascular narrowing would not resolve at a 3-month follow-up. Furthermore, atherosclerotic vascular disease frequently affects older patients, and there is often the presence of calcified vascular plaques elsewhere. Interestingly, the distribution of atherosclerosis has been shown to differ among races. Extracranial atherosclerosis is more common in Caucasians, whereas intracranial atherosclerosis is more common in non-Caucasians.
Question 2
A. Correct! The most common clinical pvresentation is a thunderclap headache (a severe headache characterized by very sudden onset), occurring in 94 to 100% of patients. This type of headache may wax and wane over minutes to days and may recur over weeks. A thunderclap headache is not entirely specific for RCVS and may also be seen in patients with aneurysmal subarachnoid hemorrhage.
The other choices are all incorrect.
Question 3
E. Correct! Posterior reversible encephalopathy syndrome (PRES), a neurologic disorder that occurs due to the inability of the cerebral circulation to autoregulate in response to insults like acute hypertension, can be seen with or without RCVS. On MRI, PRES most frequently presents as symmetric or asymmetric areas of vasogenic edema in the parietal and occipital lobes, involving the subcortical and cortical locations. However, despite being termed posterior, it can be found in other areas of the brain including the watershed or border zone territories, frontal and inferior temporal lobes, cerebellum, basal ganglia, and brainstem. Other findings include focal parenchymal hemorrhage, microhemorrhage, sulcal subarachnoid hemorrhage, and acute infarction.
Other choices and discussion
A. The imaging findings of classic progressive multifocal leukoencephalopathy are nonenhancing geographic T2 hyperintense lesions with little to no enhancement or mass effect. Lesions involve the subcortical white matter, extend into the deep white matter as the disease progresses, and are asymmetric when multifocal. Hemorrhage and vascular territory infarcts are not typically present with progressive multifocal leukoencephalopathy.
B. While posterior circulation infarcts can occur with RCVS, they are not present in every case. The appearance of hemorrhages in RCVS (when present) is also more similar to posterior reversible encephalopathy syndrome than to hemorrhagic transformation of posterior circulation strokes.
C. Although hemorrhage, edema, and infarction may occur with venous sinus thrombosis, findings related to the latter are usually confined to venous drainage territories and typically not bilateral and symmetric, as may be seen with RCVS.
D. Gliomatosis cerebri is defined by diffuse gliomatous infiltration of at least three lobes of the brain and tends to be more asymmetric than the findings in RCVS. Also, hemorrhage and infarction are typically not present with gliomatosis.
Top Tips
RCVS is a clinical and radiographic syndrome characterized by thunderclap headache, multisegmental cerebral vascular narrowing, normal blood work (erythrocyte sedimentation rate and C-reactive protein), and resolution of imaging findings within 3 months.
RCVS can occur spontaneously or can be precipitated by specific triggers (e.g., drug exposure, pregnancy complications, and postpartum state).
Complications of RCVS include sulcal subarachnoid hemorrhage, intraparenchymal hemorrhage, cerebral infarction, and PRES.
Essentials 6
Case
A 66-year-old man presents with vertigo.

Questions
1. What is the MOST likely diagnosis?
A. Dissecting pseudoaneurysm
B. Pontine hematoma
C. Choroid plexus tumor
D. Medulloblastoma
E. “Black” epidermoid
2. Which one of the following is LEAST likely to be associated with this disorder?
A. Tobacco smoking
B. Hyperlipidemia
C. Trauma
D. Extracranial internal carotid artery location
E. Larger initial pseudoaneurysm size
3. What artifact sometimes seen with nonthrombosed aneurysms is responsible for ghosting in the phase-encoding direction?
A. Susceptibility artifact
B. Aliasing artifact
C. Pulsation artifact
D. Chemical shift artifact
E. Gibbs artifact
Answers and Explanations
Question 1
A. Correct! This is a dissecting pseudoaneurysm. The large sac surrounding the intracranial segment of the right vertebral artery is consistent with a large pseudoaneurysm (left image). No gadolinium enhancement is seen within the sac on postcontrast T1-weighted image (middle image), indicating that it is largely thrombosed. This is confirmed on digital subtraction angiography (right image). The T1 hyperintensity around the periphery of the sac represents peripheral thrombus. Often, the segment or artery distal to the pseudoaneurysm or irregularly dilated segment is narrowed, and this provides a clue to the presence of a dissection. Carotid and vertebral artery dissections can result in aneurysmal dilation (pseudoaneurysms) at the site of dissection. Depending on the location, they can be fusiform or saccular in morphology. Pseudoaneurysms have the potential to enlarge, rupture, and form thrombus and embolize, leading to transient ischemic attacks and strokes. Treatment strategies are not well established but include medical management with antiplatelet or anticoagulation therapy, surgical intervention, and endovascular stenting.
Other choices and discussion
B. The lesion in this patient is extra-axial and causes mass effect on the pons, rather than arising intrinsically from the brainstem. A pontine hematoma, sometimes caused by hypertension, an underlying tumor, or a vascular malformation, would be centered within the substance of the pons.
C. Choroid plexus tumors (which include World Health Organization grade 1 choroid plexus papillomas, grade 2 atypical choroid plexus papillomas, and grade 3 choroid plexus carcinomas) are avidly enhancing intraventricular tumors. The test case lesion is not enhancing and does not originate from the ventricles.
D. Medulloblastoma is a World Health Organization grade 4 tumor that usually arises in the posterior fossa in children but can also rarely develop in adults. The location of the tumor is dependent on its molecular subgroup: the WNT (wingless) type occurs in the cerebellar peduncle/cerebellopontine angle cistern region, the SHH (sonic hedgehog) type occurs in the cerebellar hemispheres (lateral), and group 3 and group 4 types occur in the midline (fourth ventricle). Unlike medulloblastoma, the test case lesion is an extra-axial process that surrounding the right vertebral artery.
E. “Black” epidermoids have prolonged T1 values and appear “black” on T1-weighted images. They have reduced lipid content with no triglycerides or fatty acids. The presence of restricted diffusion is pathognomonic for an epidermoid, a feature that is not present in the above case.
Question 2
D. Correct! Extracranial internal carotid artery (ICA) location is the least likely of the choices provided. In one retrospective study of traumatic and spontaneous extracranial ICA dissections, dissecting pseudoaneurysms of the extracranial ICA did not grow in 90% of patients.
Other choices and discussion
A. Smoking decreases the activity of alpha-1 antitrypsin, which disrupts connective tissue integrity and results in increased pseudoaneurysm formation and enlargement.
B. Hyperlipidemia contributes to the weakening of vessel walls, promoting formation and growth of pseudoaneurysms.
C. Traumatic dissections have a higher propensity for pseudoaneurysm formation and growth than do nontraumatic and spontaneous etiologies. Traumatic cases of dissection include motor vehicle accidents (leading cause), direct assault, hanging and sporting injuries, and chiropractic neck manipulation.
E. Larger initial pseudoaneurysm size is associated with enlargement.
Question 3
C. Correct! Pulsation artifact. Pulsation of vascular structures can lead to ghosting in the phase-encoding direction. In other words, ghosts of the pulsating vessel appear at constant intervals in the phase-encoding direction. Pulsation artifact can be seen with nonthrombosed aneurysms. Similarly, loss of pulsation artifact may indicate aneurysm thrombosis.
Other choices and discussion
A. Magnetic susceptibility artifact refers to a distortion in the magnetic resonance image, often seen around metallic hardware or dental devices, due to local inhomogeneities introduced by the metallic object.
B. Aliasing artifact, also known as wrap-around artifact, occurs when the field of view is smaller than the body part being imaged. It results in spatial mismapping to the opposite side of the image. This artifact can be minimized or eliminated by oversampling the data, using surface coils, increasing the field of view, and switching the frequency and phase encoding directions.
D. Chemical shift artifact is caused by differences in resonance frequencies of fat and water. It manifests as a bright or dark outline at fat-water interfaces along the edges of an organ or lesion in the frequency-encoding direction. Fat suppression techniques can help to minimize or eliminate chemical shift artifacts.
E. Gibbs or signal truncation artifacts are ripple-like features that occur in areas characterized by abrupt transitions between regions of high and low signal intensity. They are frequently identified on T2-weighted magnetic resonance images of the spine at the interface of the low signal intensity spinal cord with the high signal intensity cerebrospinal fluid, producing a false appearance of hydromyelia.
Top Tips
Think of dissecting pseudoaneurysm when observing an irregular and dilated segment of the vertebral artery and narrowing of the vessel distally.
Treatment for pseudoaneurysms includes medical management with antiplatelet or anticoagulation therapy, surgical intervention, and endovascular stenting.
Presence of pulsation artifact can help to diagnose a nonthrombosed aneurysm; similarly, lack of pulsation artifact can indicate thrombosis of an aneurysm.
Essentials 7
Case
A 56-year-old woman presents with occasional left facial tingling and headaches.

Questions
1. What is the MOST likely diagnosis?
A. Trigeminal schwannoma
B. Cholesterol granuloma
C. Congenital cholesteatoma
D. Petrous apex cephalocele
E. Petrous apex effusion
2. This lesion represents a/an:
A. Meningocele
B. Encephalocele
C. Mucocele
D. Epidermoid cyst
E. Tumor
3. In the vast majority of cases, what is the BEST management for petrous apex cephaloceles?
A. Nothing
B. Short-term imaging follow up
C. Biopsy
D. Surgical resection
E. Radiation therapy
Answers and Explanations
Question 1
D. Correct! Petrous apex cephalocele is a rare lesion of the petrous apex representing herniation of the posterolateral aspect of Meckel cave into the petrous apex. Characteristic imaging findings of a petrous apex cephalocele include a nonenhancing unilateral or bilateral fluid signal intensity mass, arising from Meckel’s cave, with smooth erosion of the bony petrous apex. No enhancement is present in the test case (right image), although enhancement may be present if the gasserian ganglion (trigeminal ganglion) is located within the cephalocele. These lesions are often incidentally identified and are typically asymptomatic. However, if a lesion is symptomatic, surgical intervention is an option.
Other choices and discussion
A. Trigeminal schwannoma is a slow-growing tumor that originates in Meckel’s cave. It is typically hyperintense to brain on T2-weighted images and demonstrates prominent enhancement.
B. Cholesterol granuloma is the most common cystic lesion of the petrous apex, often occurring in young to middle-aged patients with a history of chronic otitis media. This lesion is typically hyperintense on T1-weighted images, and there is usually no associated enhancement.
C. Congenital cholesteatoma, also known as an epidermoid cyst, is an intraosseous lesion most frequently found in the petrous apex. It contains keratin and cholesterol. These lesions frequently restrict on diffusion-weighted imaging, a feature that is not present in this case. Congenital cholesteatomas differ from middle ear cholesteatomas, which are typically acquired secondary to perforation or rupture of the tympanic membrane.
E. An effusion can occur in pneumatized petrous apex air cells. Petrous effusions follow fluid intensity on all magnetic resonance imaging sequences and do not usually enhance. Because the test case also involves Meckel’s cave, a simple effusion as an answer choice is incorrect.
Question 2
A. Correct! Meningocele. A petrous apex cephalocele can represent either a meningocele or an arachnoid cyst, depending on the presence or absence of a dural lining (which is often difficult to identify on magnetic resonance imaging). A meningocele contains herniated dura and leptomeninges. The wall of an arachnoid cyst is comprised of arachnoid cells that form a translucent and thin membrane.
Other choices and discussion
B. An encephalocele refers to herniated brain elements, which may be dysplastic.
C. A petrous apex mucocele is similar to a mucocele found in the paranasal sinuses. It is caused by postinflammatory obstruction of pneumatized petrous air cells.
D. An epidermoid cyst, also known as a congenital cholesteatoma, is a benign intraosseous lesion most frequently found in the petrous apex.
E. A petrous apex cephalocele does not represent a tumor.
Question 3
A. Correct! Nothing. Petrous apex cephaloceles are asymptomatic, incidental findings in the vast majority of cases and require no further workup or surgical intervention. However, a small percentage of patients do have symptoms, which may include hearing loss, headaches, cerebrospinal fluid otorrhea, trigeminal neuralgia, and meningitis. Symptomatic patients have erosion of the cephalocele into the otic capsule or pneumatized petrous air cells. Surgical intervention should be considered in these cases.
Other choices and discussion
B. No further imaging is necessary for an asymptomatic and incidentally detected petrous apex cephalocele.
C. There is no role for biopsy in a petrous apex cephalocele as magnetic resonance imaging is definitive. In fact, biopsy is contraindicated and can lead to cerebrospinal fluid leaks, seizures, and meningitis.
D. Surgical treatment is only indicated when lesions erode into the temporal bone air cells, producing symptoms. In > 95% of cases, petrous apex cephaloceles are asymptomatic and incidentally detected on imaging.
E. There is no role for radiation in the treatment of petrous apex cephaloceles.
Suggested Readings
Moore KR, Fischbein NJ, Harnsberger HR, et al. Petrous apex cephaloceles. Am J Neuroradiol 2001;22:1867–1871 Razek AA, Huang BY. Lesions of the petrous apex: classification and findings at CT and MR imaging. Radiographics 2012;32:151–173Top Tips
Petrous apex cephalocele is a “DO NOT TOUCH” lesion in the vast majority of cases. Most are asymptomatic and incidentally detected.
Look for a lesion that is centered outside of the petrous apex, is contiguous with Meckel’s cave, and follows fluid signal intensity on all magnetic resonance imaging sequences.
Petrous apex cephalocele either represents a meningocele or an arachnoid cyst.
Essentials 8
Case
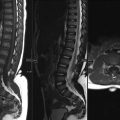
A 74-year-old man with congestive heart failure presents with back pain.

Questions
1. What is the MOST likely diagnosis?
A. Metastasis
B. Osteomyelitis
C. Osteonecrosis
D. Degenerative disease
E. Chondrosarcoma
2. On histologic analysis, the intravertebral fluid cavity (“fluid” sign) in this disorder represents:
A. Serous fluid
B. Blood products
C. Purulent fluid
D. Marrow fibrosis and edema
E. Cerebrospinal fluid
3. Which of the following is the BEST next step in management, IF the test patient experiences chronic and severe pain that is reproducible to palpation at the level of the magnetic resonance imaging findings?
A. Watchful waiting
B. Analgesics
C. Incision and drainage
D. Vertebroplasty/kyphoplasty
E. Interbody fusion
Answers and Explanations
Question 1
C. Correct! This is osteonecrosis. Osteonecrosis, or avascular necrosis, of the vertebral body is an uncommon phenomenon that occurs as the result of nonunion from postcompression fracture ischemia. “Kummel disease” represents delayed vertebral body collapse, most often involving the anterior segment of the vertebral body, after traumatic or osteoporotic nontraumatic mechanisms. Two classic imaging signs of vertebral osteonecrosis include the “vacuum cleft” sign (gaseous collections within the collapsed vertebral body appearing as very low signal intensity on T1-, T2-, and T2*- weighted images) and the “fluid” sign (fluid cavity appearing as high signal intensity on T2-weighted images and low signal intensity on T1-weighted images). The “fluid” sign located along the superior aspect of a collapsed L5 vertebral body is present in the test case.
Other choices and discussion
A. Lack of a marrow-replacing soft tissue mass argues against metastatic disease.
B. Involvement of the adjacent disc space (discitis) as well as extensive paraspinal soft tissue enhancement would be expected with bacterial osteomyelitis. Epidural and soft tissue abscesses can also be seen with discitis-osteomyelitis.
D. The “fluid” sign (as seen in the test case) is not typical for degenerative change or for any of the other diagnoses.
E. Lack of a characteristic expansile mass argues chondrosarcoma.
Question 2
D. Correct! Histologic analysis of the intravertebral fluid cavity shows reactive marrow fibrosis and edema with a high turnover rate, features indicative of osteonecrosis.
Discussion
The other choices are all incorrect. The fluid cavity does not directly communicate with the spinal canal and, therefore, does not represent cerebrospinal fluid.
Question 3
D. Correct! Aggressive treatment including vertebroplasty or kyphoplasty should be considered when intravertebral fluid is identified on magnetic resonance imaging, as treatment can prevent further collapse of affected vertebral bodies and adjacent levels. The “fluid” sign indicates formation of a cavity between viable bones that will not spontaneously heal and may become nonunited. Vertebroplasty or kyphoplasty is an effective treatment in relieving pain symptoms for patients with compression fractures, particularly those who have tenderness on exam at the level of the fracture.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


