19 | Seven Cases Illustrating the Use of Doppler Ultrasound in Obstetrics |
1—Fetal Growth Restriction
Patient A, gestational age: 29 weeks 5 days
Clinical findings: | First presentation for growth retardation of three weeks; symmetrical; mild proteinuria. Age 36; gravida 1, para 0; blood pressue (BP) normal range; cardiotocogram (CTG) normal. |
Ultrasound findings: | No evidence for malformation; estimated weight by ultrasound 1000 g (ideal weight 1400 g). |
Doppler findings: | Zero flow in umbilical a. (UA), with control (Fig. 19.1a, b); zero flow in aorta (Fig. 19.1c); brain sparing (Fig. 19.1d); bilateral uterine a. notch and abnormally raised pulsatility index (PI) (Fig. 19.1e, f). |
Assessment: | Early fetal growth restriction with impaired uteroplacental perfusion and consequent fetoplacental perfusion impairment, centralization of fetal circulation; still compensated. |
Course: | Hospitalized with bed rest until 30 weeks 4 days; BP intermittently to 160/100. At 30 weeks 6 days increasingly silent CTG showing decelerations without uterine contractions. |
Result: | Girl, 980 g; Apgar 5–8–8 (1–5–10 minutes) UA pH 7.23; base excess (BE) –4.5 mmol/L. Development good with rapid weight increase on neonatal intensive care. |
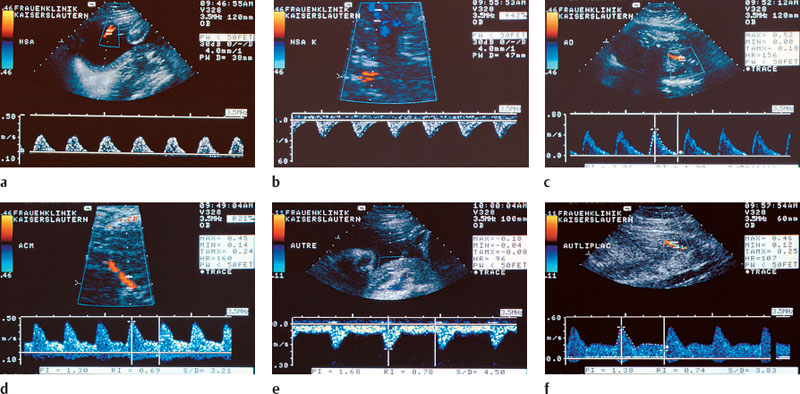
Fig. 19.1a-f Doppler ultrasound findings in a case of impaired uteroplacental perfusion with consequent impairment of fetoplacental perfusion and centralization of the fetal circulation due to early fetal growth restriction. The condition is still compensated.
a Zero flow in the UA.
b Zero flow in the UA (control),
c Zero flow in the aorta.
d Brain sparing.
e Right uterine a. with notch and abnormally elevated PI.
f Left uterine a. with notch and abnormally elevated PI.
2—Extreme Fetal Growth Restriction Due to Endarteritis Obliterans
Patient B, gestational age: 28 weeks 3 days
Clinical findings: | Age 22, gravida 2, para 0, status post intrauterine death at 18th week of pregnancy two years ago. Initial presentation for oligohydramnios; CTG shows silent oscillations. |
Ultrasound findings: | Extreme growth retardation of six to seven weeks, anhydramnios, estimated weight by ultrasound < 300 g; mild pericardial effusion. |
Doppler findings: | Zero to reverse flow in the UA (Fig. 19.2a); zero flow in the aorta (Fig. 19.2b); brain sparing (Fig. 19.2c); abnormal flow in the inferior vena cava (IVC) (Fig. 19.2d); uteroplacental flow unremarkable (Fig. 19.2e). |
Assessment: | Unfavorable prognosis due to extreme maldevelopment. No clear obstetric basis for decision concerning the child. Consultation included mother and pediatrician, consensus regarding expectant treatment. |
Course: | After three days intrauterine death confirmed; prostaglandin induction. |
Result: | Spontaneous delivery 290 g; no malformation; placenta shows severe endarteritis obliterans. |
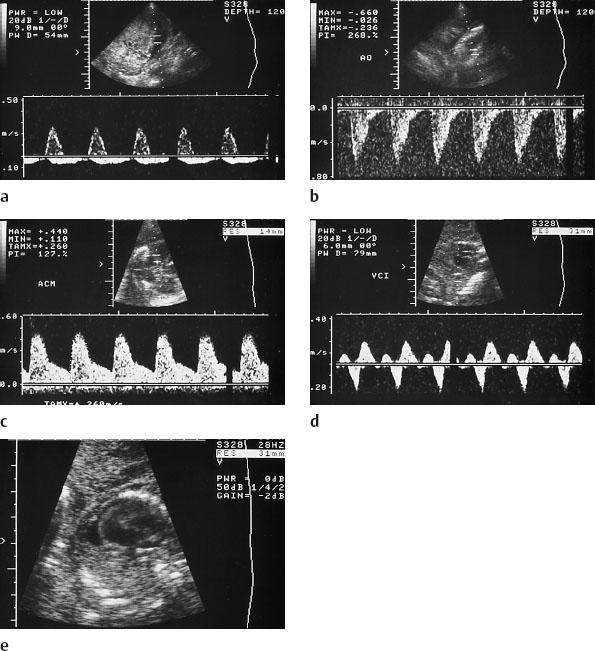
Fig. 19.2a-e Doppler ultrasound findings in extreme growth restriction with poor prognosis.
a Zero and reverse flow in the UA.
b Zero flow in the aorta,
c Brain sparing.
d Abnormal flow in the IVC.
e No abnormal finding in uteroplacental flow.
3—Exclusion of Potter Syndrome
Patient C, gestational age: 26 weeks 4 days
Clinical findings: | Age 26, gravida 1, para 0. First presentation for suspected Potter syndrome due to decreased amniotic fluid. |
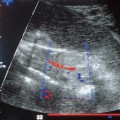
Ultrasound findings: | Anhydramnios, disproportional growth restriction, head diameters appropriate to gestational age, thorax retarded by two weeks, weight estimated by ultrasound 800 g; kidneys were displayed by color Doppler bilaterally (Fig. 19.3a, b). |
Doppler findings: | Reverse flow in the UA (Fig. 19.3c); reverse flow in the aorta (Fig. 19.3d); brain sparing (Fig. 19.3e); abnormal uteroplacental perfusion bilaterally with notch (Fig. 19.3f, g). |
Evaluation: | No Potter syndrome; severe uteroplacental and fetoplacental perfusion impairment with centralization of the circulation. |
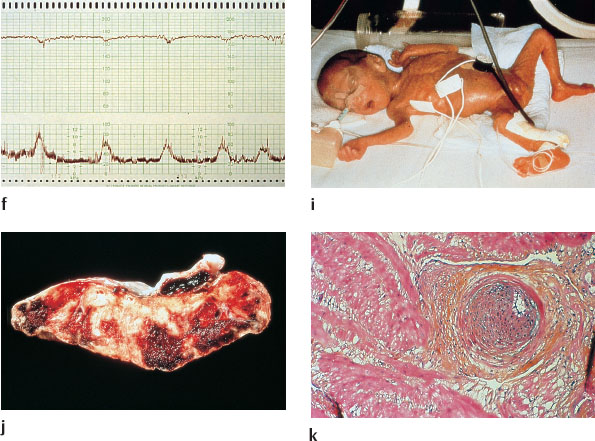
Course: | Evening CTG showed “bird’s wing” pattern (i. e., CTG looks like the silhouette of birds flying as seen from a distance; a typical CTG pattern correlated to fatal hypoxia) with silent oscillation and spontaneous contractions (Fig. 19.3h). Emergency section with biopsy of the placental bed (i.e., uterine tissue adjacent to placental insertion). |
Result: | 760 g, no malformations (Fig. 19.3i). Apgar 4 (1 minute): primary intubation UA pH 7.18, BE –10 mmol/L. |
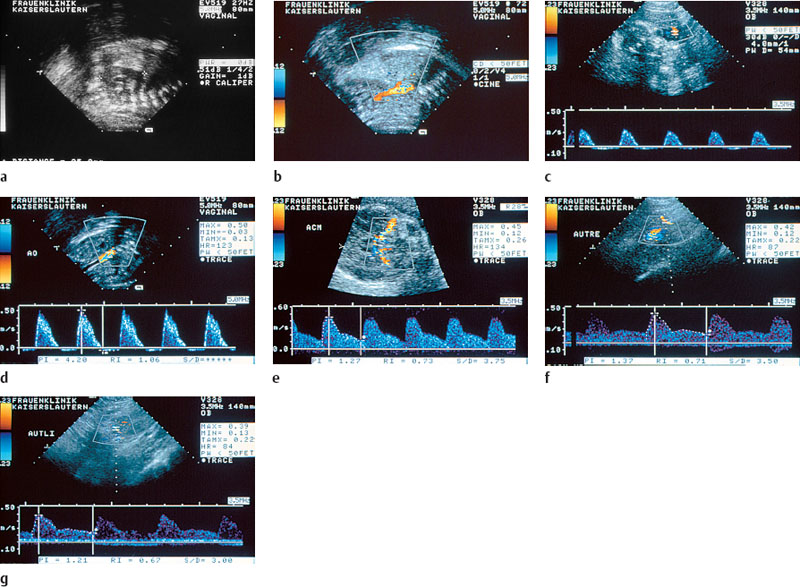
Fig. 19.3a-k Fndings in severe impairment of uteroplacental and fetoplacental perfusion with centralization of the circulation.
a Sonographic image of a fetal kidney.
b Color Doppler image of renal arteries.
c Reverse flow in the UA.
d Reverse flow in the aorta.
e Brain sparing.
f Abnormal perfusion with notch in the right uterine a.
g Abnormal perfusion with notch in the left uterine a.
h CTG. “Bird’s wing” pattern with silent oscillation
i Newborn infant, 760 g, Apgar4, primary intubation required.
j Placenta showing old and more recent infarctions, in total 80% in-farcted.
k Placental bed biopsy histology shows predominantly eccentric narrowing of the lumen and occlusion of the spiral arteries, media hypertrophy, and proliferation of fibroblasts.
4—Closely Coordinated Preventive Care for High-Risk Patients
Patient D, gestational age: 6–38 weeks