Skull Fractures
Ken F. Linnau
John H. Harris Jr.
CONTEXT AND EPIDEMIOLOGY
Since ancient times, humans are believed to have treated trauma to the head and skull. Anthropologic evidence suggests that the Incas in Peru have used trepanation techniques for treatment of skull fractures as early as 200 BC, and current treatment techniques have evolved from the observations and practices of Greek and Roman physicians.1,2
This chapter illustrates and describes the imaging characteristics of acute injury of the cranial bones at the initial patient encounter in the emergency center. The true incidence of skull fractures in children and adults presenting to emergency departments (ED) is unknown and much of the data is derived from traumatic brain injury (TBI) evaluation, which affects about 1.7 million patients every year and accounts for up to 1.4 million annual ED visits in the United States (2006 data).3 About 300,000 TBI patients are hospitalized annually and about 4% of patients treated for head trauma have a skull fracture.4 The most common causes of TBI include falls (35%), motor vehicle crashes (MVC) (17%), assaults (10%), and being struck by or against an object. Falls show the highest rates in children less than 4 years and adults older than 75 years of age. MVC injury is the leading cause of TBI-related death, particularly in young adults who are less than 24 years old.
In children, intentional injury (i.e., non-accidental trauma, abusive head trauma) represents an important cause of skull fractures and associated morbidity such as intracranial hemorrhage and retinal bleeding.5
INDICATIONS FOR IMAGING AND SUPPORTING EVIDENCE
Indiscriminate use of skull radiographs triggered one of the earliest assessments for rational imaging use. In 1987, a prospective study of ED patients was performed to validate an expert guideline, which recommended that low-risk patients should not undergo routine skull radiography after head trauma in order to reduce radiation exposure and imaging cost.6,7 Today, computed tomography (CT) is the imaging modality of choice in the initial evaluation of patients with emergent cranial and intracranial signs and symptoms. The need for imaging is usually based on the severity of head injury as indicated by initial Glasgow Coma Scale (GCS) (Table 1.1). With this scale, the three main aspects of neurologic function evaluated are (1) opening of the eyes to external stimuli, (2) verbal response, and (3) motor response to stimuli. Strong evidence supports the use of urgent head CT imaging for severe TBI (based on a GCS of 3 to 8) to identify lesions requiring surgical intervention. Clinical prediction rules, such as the Canadian Head CT rule and the New Orleans criteria, derived and validated using sophisticated scientific methodology inform evidence-based imaging recommendations with CT for mild TBI. The reader is directed to the
original citations for details.8,9 Tong et al. have recently summarized the available evidence guiding imaging for TBI.10
original citations for details.8,9 Tong et al. have recently summarized the available evidence guiding imaging for TBI.10
TABLE 1.1 Glasgow Coma Scale | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the initial assessment of any trauma patient, rapid identification and stabilization of life-threatening traumatic injuries is the primary goal. Airway protection and control of bleeding are mandated during this primary survey. To control bleeding from scalp lacerations, it is sometimes necessary to staple them closed in the prehospital setting to obtain adequate hemostasis.
Identification of skull fractures increases the chance of detecting associated cervical spine injuries to 15% or more, mandating prehospital spine precautions and careful evaluation of the craniocervical junction.
Radiography
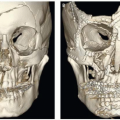
Radiographs previously played a major role in the evaluation of skull and brain lesions but now have a very limited role for the evaluation of skull fractures and are superfluous if a CT of the head has been obtained. For depiction of linear skull fractures, which may be overlooked on axial CT images, scout view images (topograms), which are included in every CT scan, can be used as a substitute for radiographs (Figs. 1.1, 1.3, and 1.4) or 3D renderings from CT (Figs. 1.2, 1.3, 1.4 and 1.5




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
