Anatomy, embryology, pathophysiology
Please see Chapter 33 .
Imaging techniques and protocols
Please see Chapter 33 .
Specific disease processes
A purely solid adnexal lesion is usually considered benign, with a few exceptions. This chapter provides a differential for benign and malignant solid adnexal lesions with emphasis on their imaging appearances. However, it is worth noting that the most common ovarian tumors are epithelial ovarian tumors, which are predominantly cystic or part solid and cystic (see Chapter 33 ).
Benign solid adnexal masses
Ovarian fibroma
Fibromas and fibrothecomas are the most common solid ovarian tumor in asymptomatic women of all ages. They are considered an ovarian stromal tumor and are almost universally hormonally inactive.
Fibromas may be associated with ascites or pleural effusions, a constellation of findings known as Meig syndrome. They also have a strong association with basal cell nevus syndrome (Gorlin Goltz syndrome) and are seen in up to 75% of female patients.
Ultrasound
- ■
Typically a solid hypoechoic mass, commonly unilateral.
Magnetic resonance imaging
- ■
T1 and T2 hypointense, well-circumscribed solid masses with mild enhancement ( Figs. 34.1 and 34.2 ).

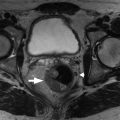
Fig. 34.1
Ovarian fibroma. Axial T2-weighted image (A) shows a small left ovarian fibroma ( arrow in A) with very low signal and mild enhancement ( circle in B) in the T1-weighted fat-suppressed enhanced image (B).
(From Roth C, Deshmukh S. Fundamentals of Body MRI , ed 2. Philadelphia: Elsevier; 2016.)

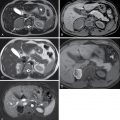
Fig. 34.2
Bilateral fibromas. Serpiginous hypointensity ( arrows ) distorts the appearance of the ovaries bilaterally in axial (A) and coronal (B) T2-weighted images. C, Axial T1-weighted in-phase gradient echo image shows monotonous mild hypointensity to isointensity ( circles ), and signal characteristics most strongly suggest fibrous tissue. D, Mild bilateral enhancement ( circles ) is noted in the subtracted postcontrast image.
(From Roth C, Deshmukh S. Fundamentals of Body MRI , ed 2. Philadelphia: Elsevier; 2016.)
Pedunculated fibroid
This is a subserosal fibroid that projects exophytically to produce a parauterine mass. A pedunculated fibroid is difficult to differentiate from a fibroma ( Fig. 34.3 ). A helpful clue is to look for a “bridging vessel” sign. This is the demonstration of flow voids of the uterine artery extending to the lesion. Fibroids typically demonstrate marked postcontrast enhancement, unless there is myxoid degeneration, where it is T2 hyperintense and relatively hypoenhancing.

Brenner tumor
This is an uncommon epithelial ovarian tumor. Brenner tumors were previously referred to as transitional cell tumors as their histopathologic appearance was similar to urothelium. In up to 30% of cases, a Brenner tumor is associated with an additional epithelial neoplasm in the same or other ovary. Brenner tumors are most commonly seen in women in their fifth and seventh decades.
Ultrasound
- ■
Hypoechoic mass ± calcifications (up to half of lesions).
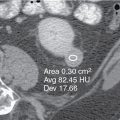
Computed tomography
- ■
Solid lesion with mild postcontrast enhancement and calcification.
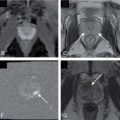
Magnetic resonance imaging
- ■
T2 hypointense, fibrous tumor ( Fig. 34.4 ).