Figure 5.1.1
Meningomyelocele. A: Coronal image of spine with meningomyelocele demonstrating disruption of lower spine (arrows) and protrusion of a cystic mass (arrowheads) representing the dorsal sac. B: Sagittal image of another fetus with lumbosacral spinal defect showing opening of the distal spine (arrows) with cystic mass protruding posteriorly (arrowheads). C: Three-dimensional ultrasound with skeletal setting demonstrating widening of the distance between the posterior elements in the lower lumbar and upper sacral spine (arrows) due to spina bifida.
The fetal head is abnormal in most fetuses with meningomyeloceles. The posterior fossa is small, and the cerebellum is compressed against the occiput, obliterating the cisterna magna. During the second trimester, the small cerebellum is hypoechoic and curved around the cerebellar peduncles, with an appearance called the “banana” sign (Figure 5.1.4). Later in pregnancy, the cerebellum is larger and more echogenic, although it is still compressed against the occiput, and no fluid will be seen in the region of the cisterna magna.
Hydrocephalus, with dilation of the lateral ventricles, is present in the majority of cases of meningomyelocele and the Chiari II malformation.

 Figure 5.1.2
Figure 5.1.2
Meningomyelocele with splaying of posterior ossification centers. A: Transverse image of spine at level of meningomyelocele demonstrating marked splaying of the two posterior ossification centers (arrows). The third ossification center between the two represents the vertebral body. A large dorsal sac protrudes posteriorly (arrowheads). B: Transverse image of meningomyelocele in another fetus demonstrating widened posterior ossification centers (arrows) and a complex cystic mass protruding from the defect (arrowheads).

Figure 5.1.3
Dorsal sac: Three-dimensional (3D) view. A and B: 3D images demonstrating a cystic mass (arrows) protruding posteriorly from the back of a fetus with a meningomyelocele.

Figure 5.1.4
Banana sign associated with meningomyelocele. Axial image of posterior fossa demonstrating banana-shaped cerebellum (arrows) in a small posterior fossa with effacement of the cisterna magna, due to the Chiari II malformation. This fetus had a lumbosacral meningomyelocele.
During the second trimester, the cranium of most fetuses with meningomyeloceles has an abnormal contour termed the “lemon” sign. This is characterized by flattening or concavity of the frontal bones (Figure 5.1.5). By the third trimester, the cranium is more ossified and develops a normal oval configuration.
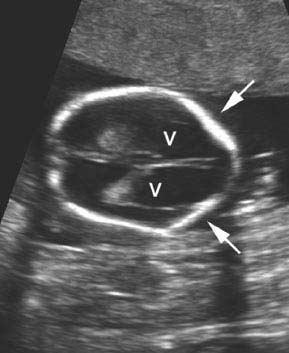
Figure 5.1.5
Lemon sign. Axial image of head in a fetus with meningomyelocele demonstrating flattening of the frontal bones (arrows) giving the head a lemon shape. The lateral ventricles (V) are dilated.
The spinal defect with meningoceles is typically smaller than with meningomyelocele, as is the dorsal sac. The sac of the meningocele is seen as a cystic lesion protruding posteriorly from a narrow opening in the spine (Figure 5.1.6). The posterior fossa appears normal, because the Chiari II malformation is not present.

 Figure 5.1.6
Figure 5.1.6
Thoracic meningocele. A: Sagittal image of thoracic spine demonstrating a cystic mass (arrow) protruding posteriorly, representing a thoracic meningocele. B: The posterior fossa in the same fetus appears normal with a normal shaped cerebellum (arrows). C: Sagittal image in another fetus with thoracic meningocele demonstrating the cystic mass (arrows) protruding through a spinal defect. D: Three-dimensional image demonstrating the same posterior cystic mass (arrow).
5.2. Hemivertebra
Description and Clinical Features
A hemivertebra is an anomalous vertebra in which part or all of one side of the vertebral body and posterior elements is absent. The result is a kink or bend in the spine at the affected level, causing scoliosis. The anomaly can affect a single or multiple vertebrae. Affected vertebral bodies have a wedge shape. Associated anomalies of the skeletal system are common, most often involving the ribs and extremities. In addition, hemivertebra is a component of various syndromes with anomalies affecting many organ systems, including the cardiovascular, gastrointestinal, central nervous, and genitourinary systems. The prognosis depends on the degree of severity of the associated anomalies.
Sonography
On ultrasound, a hemivertebra is seen on a coronal view of the spine as a disruption of the normally paired posterior ossification centers. An extra posterior ossification center will be seen on one side, without a matching ossification center on the other (Figure 5.2.1). In addition, a kink or bend in the spine will be identified at that level. Hemivertebrae are often well visualized using three-dimensional (3D) ultrasound with skeletal settings (Figure 5.2.2).
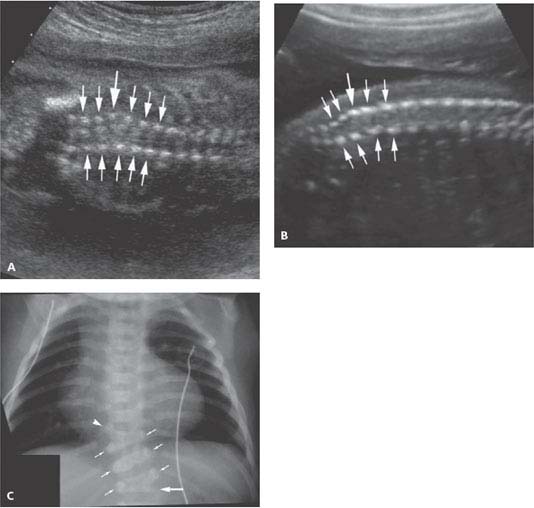
Figure 5.2.1
Hemivertebrae. A and B: Longitudinal images of lower thoracic and upper lumbar spine demonstrating a kink in the lower spine at the site of an extra ossification center on one side (large arrow) representing a hemivertebra. The posterior ossification centers (small arrows) for the other vertebral bodies correspond one-to-one. C: X-ray of neonate with hemivertebra (large arrow) imaged after birth. Matched posterior ossification centers (small arrows) are seen superiorly. A second contralateral hemivertebra (arrowhead) is noted three levels above.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


