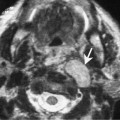
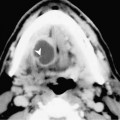
Chapter 56 Squamous cell carcinoma (SCCA) of the palatine tonsil accounts for between 1.5 and 3.0% of all cancers of the upper aerodigestive tract. This is second only in incidence to laryngeal carcinomas in this region. Men are affected more than women. The peak incidence is in the seventh decade in men and the sixth decade in women. The most common risk factors are excessive tobacco and alcohol use. The clinical findings are nonspecific and may often be subtle. The stages of SCCA have been classified by the American Joint Committee on Cancer (Table 56–1). The initial symptom may only be a sore throat. However, the presence of a sore throat plus otalgia should increase the suspicion of an underlying malignancy. Many patients will initially present with a neck mass. The palatine tonsil is a common location for patients that have neck metastases but no visible lesion (Fig. 56–1). This is referred to as an unknown primary tumor. Many institutions perform a tonsillectomy on the side of the nodal metastases due to the high likelihood of metastases from early tonsillar carcinomas. In fact, > 70% of patients with tonsillar carcinomas will present with neck metastases at initial examination. The primary echelon lymph nodes are to the ipsilateral jugular chain and the retropharyngeal lymph nodes. The spinal accessory and submandibular groups are also at risk. Tumors that extend inferiorly to the tongue base or superiorly to the soft palate attain the lymphatic drainage of these subsites. Contralateral involvement is less common, occurs in approximately 10% of cases, and is usually associated with spread to these areas. The majority (> 90%) of epithelial neoplasms of the tonsil are squamous cell carcinoma. These tend to be undifferentiated or anaplastic tumors that metastasize early. Early T1 and T2 lesions that do no extend through the visceral fascia into the parapharyngeal space can be treated with definitive RT or a wide local excision using a transoral approach. The surgical treatment for advanced tumors may be resected using a mandibular swing approach for tumors that are not adjacent to the mandible. The surgical resection for larger tumors that are adjacent to the mandible require a segmental mandibulectomy and partial glossectomy followed by reconstruction. The primary treatment option for nonsurgical organ preservation for advanced tumors is combined chemotherapy and radiation therapy.
Squamous Cell Carcinoma of the Palatine (Faucial) Tonsil
Epidemiology
Clinical Features
Pathology
Treatment
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


