| CRANIAL REGION | Superior sagittal and transverse sinuses |
| HISTOPATHOLOGY | Meningioma, meningothelial type, WHO grade I |
| PRIOR SURGICAL RESECTION | Yes |
| PERTINENT LABORATORY FINDINGS | N/A |
Case description
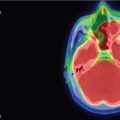
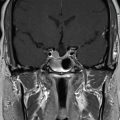
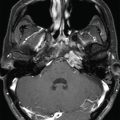
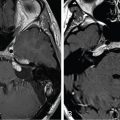
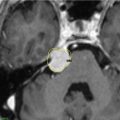
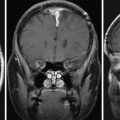
A 55-year-old female presented with a headache, gait ataxia, and a right inferior visual field defect. Magnetic resonance imaging (MRI) demonstrated a large left parasagittal meningioma that invaded the sagittal and transverse sinuses bilaterally, resulting in midline shift and extensive left hemispheric edema. Angiography confirmed occlusion of the superior sagittal sinus (SSS) and torcula by the tumor ( Figure 12.57.1 ). The patient underwent multimodality management, including embolization followed by subtotal resection of the parasagittal mass. Pathology revealed a WHO grade 1 meningothelial meningioma.

Images obtained at 2 months after resection demonstrated progression of the tumor. Stereotactic radiosurgery (SRS) was offered as an adjunct to surgery to control tumor progression. This tumor had a large volume; therefore, staged SRS was recommended to reduce the chances of adverse radiation effects while maintaining tumor control. SRS was performed in three stages over a 3-month interval. A marginal dose of 12.5 Gy was delivered to the 50% isodose line during each volume-staged SRS ( Figure 12.57.2 ). This was followed by a boost-fractionated intensity modulated radiation therapy (IMRT) (54 Gy, 20 fractions). The tumor remained stable for 9 years. A decade after the initial craniotomy, the patient presented with new tumor progression with cerebellar edema. In view of the high risk of morbidity with additional resection of this complex tumor, repeat SRS was offered as a minimally invasive option to prevent further progression. She underwent repeat SRS (11 Gy at the 50% isodose line), and bevacizumab therapy was initiated (see Figure 12.57.2 ).
| Radiosurgery Machine | Gamma Knife – Model C |
| Radiosurgery Dose (Gy) |
|
| Number of Fractions |
|
Related posts:
 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chondrosarcoma – definitive radiosurgery after subtotal resections
Chondrosarcoma – definitive radiosurgery after subtotal resections
 Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
 Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


