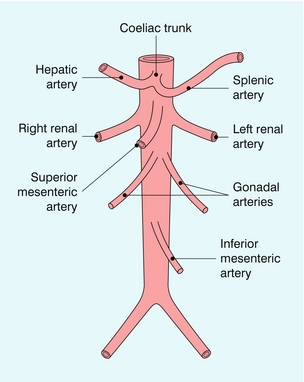
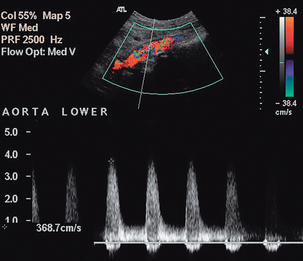
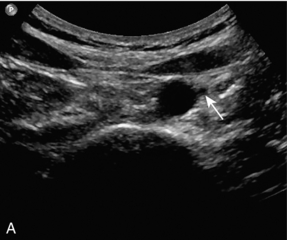
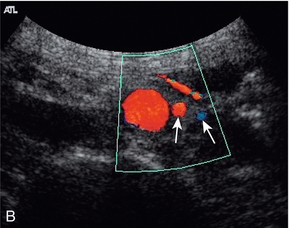
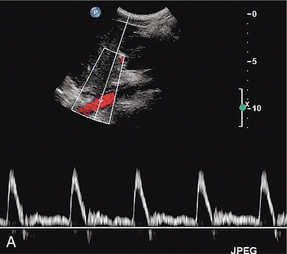
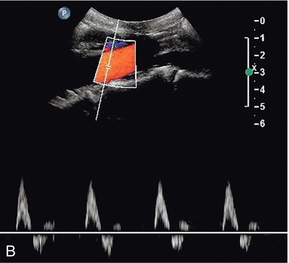
Chapter 6 Abdominal Doppler examinations are performed on vessels which lie more deeply than the peripheral vessels and this has several consequences. First, lower-frequency transducers are used and this limits the size of Doppler shift which will be obtained for a given velocity. Second, longer-pulse repetition intervals are required to allow the sound to travel the greater distances; this also limits the size of Doppler shift which can be measured as a result of the Nyquist limit (see Chapter 1). Operators should therefore seek to minimise the scan depth and use the highest-frequency transducer compatible with adequate visualisation. The abdominal aorta gives branches to the abdominal organs and to the abdominal wall. The parietal branches to the abdominal wall are not usually large enough to be seen regularly using colour Doppler and will not be considered further. The visceral branches (Fig. 6-1) supply the liver, kidneys, adrenal glands, gonads, spleen, bowel and pancreas. The vessels to the adrenals and gonads are also usually too small to be seen reliably on ultrasound; the renal, hepatic and iliac arteries are covered elsewhere in greater detail. The splanchnic arteries supply the bowel and associated organs. The coeliac trunk (Fig. 6-2) arises from the anterior aspect of the aorta just after it has entered the abdomen. The trunk is only about 1 cm long and divides into three branches: the common hepatic artery, the splenic artery and the left gastric artery. The common hepatic artery passes to the right over the head of the pancreas, where it gives off the gastroduodenal artery which can be seen passing inferiorly between the head of the pancreas and the margin of the duodenum; the other branches from this segment of the hepatic artery are not usually apparent on ultrasound. The artery ascends in the lesser omentum as the proper hepatic artery, in company with the portal vein and common bile duct, to the porta of the liver, where it divides into right and left hepatic arteries. The splenic artery passes to the left and runs along the superior margin of the body of the pancreas to the hilum of the spleen. It has a tortuous course and an arterial loop may be mistaken for a small cyst in the pancreas if the situation is not recognised; colour Doppler allows quick identification of the true nature of the ‘cyst’. The right gastric artery arises from the splenic artery but is not usually seen on ultrasound. FIGURE 6-2 Transverse view of the coeliac axis showing the splenic artery on the right and the hepatic artery on the left. The superior mesenteric artery (Fig. 6-3) arises 1–2 cm below the coeliac trunk and supplies the small bowel and colon to the distal transverse colon. The superior mesenteric vein is seen on the right side of the upper portion of the artery and can be followed to its confluence with the splenic vein, forming the portal vein. The individual branches of the superior mesenteric artery are not usually seen clearly on ultrasound. The inferior mesenteric artery (Fig. 6-4) arises from the anterior aorta about 3–4 cm above the bifurcation and runs inferiorly to the left side of the aorta. The inferior mesenteric vein may be seen on the left of the artery but diverges as it passes up to join the splenic vein. FIGURE 6-3 Longitudinal scan showing the origin of the coeliac axis superiorly and the superior mesenteric artery just below this. Colour Doppler shows aliasing and a tissue bruit around a stenotic coeliac axis origin. FIGURE 6-4 (A) Transverse scan showing the inferior mesenteric artery lying adjacent to the aorta (arrow); (B) colour Doppler image showing the inferior mesenteric artery and vein (arrows). The coeliac trunk and its main branches are examined using colour and spectral Doppler. The main trunk is short but it is directed towards the transducer so that an excellent Doppler angle is achieved. The proximal hepatic and splenic arteries, together with the superior mesenteric artery, are often orientated almost at right angles to the transducer with an anterior approach (Fig. 6-2), so that some experimentation with points of access is required to get acceptable Doppler angles. The hepatic artery is followed to the right and the gastroduodenal artery can be identified beside the head of the pancreas. The proper hepatic artery is traced towards the porta where it divides into the right and left hepatic arteries. The origin of the superior mesenteric artery is examined (Fig. 6-3) and the vessel traced as far distally as it remains visible. Firm pressure with the transducer may help in displacing bowel gas from in front of the vessel, but care must be taken not to compress the artery and produce a spuriously high Doppler shift. Colour Doppler is used to identify any abnormal areas of flow, including ‘visible bruits’, or tissue vibrations, which may be seen in cases of severe stenosis (Fig. 6-3). Power Doppler is of less value in the abdomen than in peripheral vessels as arterial pulsation, respiratory movement and bowel gas motion can all cause marked motion artefacts which obscure the signal from the vessel. The inferior mesenteric artery is sometimes difficult to locate. It can be found by scanning transversely up from the bifurcation and it may be identified just to the left of the aorta, 2–4 cm above the bifurcation (Fig. 6-4). The calibre of the normal aorta varies with the age, sex and build of the patient, being larger in men, older patients and tall patients. The calibre also varies with the level in the abdomen. Goldberg et al. found an average diameter of 22 mm above the renal arteries, 18 mm just below the renal arteries and 15 mm above the bifurcation.1 The normal Doppler waveform in the aorta also varies with location. In the upper aorta there is a narrow, well-defined systolic complex with forward flow during diastole; below the renal arteries the diastolic flow is much reduced and above the bifurcation it is absent, or reversed diastolic flow may occur, with a waveform similar to that seen in the lower limb arteries (Fig. 6-5).2 FIGURE 6-5 (A) The aortic waveform in the upper abdomen showing diastolic flow. (B) The aortic waveform above the bifurcation with absent diastolic flow and a waveform similar to that seen in the lower limb arteries. The main abnormalities affecting the aorta are atheroma, aneurysm, dissection and para-aortic masses. Atheroma can affect the aorta and produce stenosis (Fig. 6-6), or occlusion; aortic disease, unless severe is usually overshadowed clinically by symptoms arising from the peripheral or the coronary arteries. Sometimes there is uncertainty as to whether aortic disease seen on arteriography is clinically significant. In these cases velocity ratios taken from above and at the stenosis can be used to assess the degree of haemodynamic compromise. However, accurate criteria are not as fully developed for aortic stenosis, unlike the situation for carotid and peripheral Doppler examinations; however, in one study3 a peak systolic velocity ratio of 2.8 correlated (86% sensitivity, 84% specificity) with aortoiliac stenoses of > 50% diameter reduction and a ratio of 5.0 showed some correlation (65% sensitivity, 91% specificity) with stenoses > 75%. If the stenotic area is clearly seen, a direct measurement of diameter or area stenosis may be obtained; colour or power Doppler is of value in defining the margins of the residual lumen.
 The Aorta and Inferior Vena Cava
The Aorta and Inferior Vena Cava
The Aorta
ANATOMY
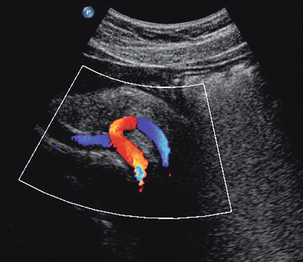
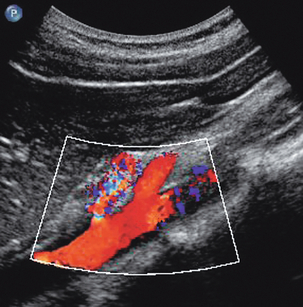
SCANNING TECHNIQUE
Splanchnic Arteries
NORMAL AND ABNORMAL FINDINGS
Aorta
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The Aorta and Inferior Vena Cava