Endoscopy with biopsy and/or microbiological investigation is a definitive tool for the diagnosis of colonic diseases, whether inflammatory or tumoral. However, imaging techniques remain essential in the evaluation of some entities like:
Anorectal anomalies: atresia with or without fistulas (contrast examinations, US, and MR to determine its level and the presence of fistulas). Radiograph neither useful nor diagnostic.
Hirschsprung disease: a well-done low-pressure enema may detect the transition zone between the distal aganglionic segment and the proximal dilated colon, otherwise it is diff cult to assess even with biopsy
Appendicitis: US has high accuracy without radiation risks.
Plain X-ray: similar to other forms of low SBO. Barium enema (lateral view): transition zone between the normal or relatively narrow aganglionic segment and the dilated bowel proximal to it.
Low intestinal obstruction caused by the absence of normal myenteric ganglion cells in a segment of the colon.
Abdominal distention, failure to pass meconium in the first 24 h of life, constipation, and bilious vomiting are the predominant symptoms.
Large amounts of air mixed with stools throughout the entire large bowel. Acquired fecal retention, especially in the sigmoid colon and rectum.
Most common cause of colonic dilatation in infancy and school-age children. Causes: diff cult toilet training, neuropsychogenetic abnormalities, hypothyroidism, malnutrition, etc.
Toxic megacolon
Marked dilatation of the transverse colon in particular. Nodular thickening and rigidity of the colonic wall. Increased perforation risk: air-fluid levels and ascites.
Infrequent complication of ulcerative colitis and other colitis. Enema is contraindicated.
Fig. 2.107a, b Hirschsprung disease. Anteroposterior (a) and lateral (b) views of a contrast enema show the significant dilatation of the sigmoid and proximal rectum. The distal rectum is not dilated, representing the aganglionic segment.Fig. 2.108 Colon atresia. Contrast enema shows abnormally small colon (microcolon) with complete obstruction to retrograde flow of contrast material proximal to the middle transverse portion of colon (arrow). There is gaseous distention of proximal bowel.Fig. 2.109 Chronic constipation. Plain abdominal film shows colonic distention by feces that occupies all the segments.Fig. 2.110 Fecaloma. Plain abdominal film shows fecaloma in rectum outlined by gas in a girl with abdominal pain and with no evacuation in the last 10 days.Fig. 2.111 Chilaiditi syndrome. Plain abdominal films shows transverse colon interposition between the liver and the anterior abdominal wall. Nasoduodenal tube is seen.
Abdominal X-ray: linear or cystic pneumatosis intestinalis (submucosal or subserosal air). Portal vein gas: finely branching radiolucencies extending from the porta hepatis to the periphery of the liver.
US: bright, shifting echogenic foci within the portal vein.
In premature infants weighing < 1500 g. Factors: ischemia, decreased mucus production, diminished immune response of the premature infants, Hirschsprung. Complications: perforation, strictures.
Crohn: Asymmetric changes in the wall. Skip lesions and fistulas.
Crohn: more frequent in the ileocecal region.
DD: TB and amebic dysentery. Ulcerative colitis begins in the rectum and ascends. Fistulas are very rare.
Pseudomembranous enterocolitis
Marked thickening of the colon wall. Mucosal irregularity and ulcerations. Pseudomembranes on contrast studies.
Complication of oral antibiotic therapy. Caused by Clostridium diff cile.
Hemolytic uremic syndrome
Thickening of the colon with irregular narrowing of the lumen and “thumbprinting” pattern due to intramural hemorrhage. Lost of bowel wall layering.
Hemolytic anemia, renal failure, and thrombocytopenia. DD: Henoch-Schönlein purpura predominates in the small bowel and shows flow on Doppler US. US examination of the kidneys.
Secondary to inflammatory intestinal disease, adenomatous polyposis, sporadic.
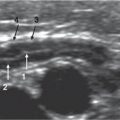
Fig. 2.112 Pneumatosis intestinalis in a 1-week-old infant. Antero-posterior plain radiograph shows small and large bowel loops sharply outlined by collections of air in bowel wall (arrows). Most of these collections of air are linear, suggesting a submucosal location.Fig. 2.113 Necrotizing enterocolitis. Longitudinal US scan at the transverse colon shows air bubbles (arrows) within the colonic wall corresponding to pneumatosis intestinalis.Fig. 2.114a, b Pneumoperitoneum complicating necrotizing enterocolitis. (a) Supine radiograph in a 1-month-old premature infant shows intramural air in the small bowel and free intraperitoneal air secondary to bowel perforation. The central lucency and the falciform ligament are seen (“football” sign). (b) Horizontal beam decubitus radiograph in another patient that shows pneumoperitoneum (arrows) due to bowel perforation in a premature infant.Fig. 2.115 Portal vein air. Plain radiographs: air is observed within the portal vein branches, complicating pneumatosis intestinalis in a 3-week-old premature infant.Fig. 2.116a, b Portal vein air. (a) Transverse sonogram of the liver shows multiple echogenic areas (arrows) corresponding to air within the portal vein branches. (b) Air is also observed within the hepatic veins.Fig. 2.117 Salmonellosis. Axial Doppler US through the transverse colon depicts a hypervascularized thickened colonic wall with a patent hyperemic submucosal layer.Fig. 2.118 Ulcerative colitis. Longitudinal US ultrasound through the left colon: The normal folds are lost and the lumen is filled with fluid. This is the US counterpart of the “lead-pipe” appearance on a contrast enema.Fig. 2.119 Retrocecal appendical abscess. Axial Doppler US: A fluid collection with high-level echoes and with hypoechoic thick wall is seen in the retrocecal area (between the abdominal muscular wall and the right kidney posteriorly). Doppler signal is depicted in the abscess wall.Fig. 2.120 Inflamed appendiceal stump. Axial US image through cecal area shows a multilayered image (arrowhead; bowel inside bowel) due to the remaining inflamed submucosa in the invaginated appendiceal stump (tobacco bag).Fig. 2.121a, b Sigmoid hemangiomatosis. B-mode (a) and Doppler (b) US through the left iliac fossa show a sigmoid colon with parietal thickening and hypoechoic areas with prominent flow.Fig. 2.122a, b Colon lymphoma. A 6-year-old boy diagnosed with intussesception with a pathologic lead-point by US. A saline enema was performed, achieving full reduction. (a) The postreduction US image shows a hypoechoic homogenous mass in the anterior wall of the ascending colon. The mass was biopsied and diagnosed as Burkitt lymphoma. (b) The CT image depicts a hypoattenuating mass with no lymphadenopathies or other findings present. This procedure avoided the necessity to perform a partial colectomy.Fig. 2.123 Intussuscepted sigmoid carcinoma. A 12-year-old boy with constipation and rectal mass at examination. CT examination with rectal contrast depicts a parietal colonic mass with mucosal irregularity and outlined with contrast. This mass is the lead-point of a sigmoid-rectal intussesception: the crescent-shaped intussuscepted mesentery is depicted.
Table 2.55 Anorectal anomalies in neonates
Diagnosis
Findings
Comments
High anomaly without fistula
Blind-ending pouch above the I-point (lowest point of the pubis or below the tip of the ischium). Voiding cystourethrogram (VCUG).
Demonstration of fistula with VCUG in boys or contrast filling from the anus in girls.
May present with air in bladder or meconium in urine.
Perineal and vulvar fistulas
Retrograde contrast evaluation.
Always low anomalies.
Transscrotal fistulas
Retrograde contrast evaluation.
Intermediate anomaly.
Fig. 2.124a, b Anal atresia. (a) Sagittal US in transperineal approach shows the blind-ended rectum filled with meconium (hyperechoic dots). The calipers measure the distance between rectum and perineal surface. (b) Axial US from the posterior shows the normal muscular pelvic anatomy, which is encircling the rectal pouch.Fig. 2.125 Anal atresia, postoperative. Axial T1 MRI with a rectal tube inserted, which helps to evaluate the proper position of descended rectum. In this case, the rectum is slightly lateralized to the left.
Table 2.56 The colon: Diverticula and duplications
The cecum accounts for about 40% of cystic colonic duplications, and its imaging features are similar to those of small bowel duplications.
US: a cystic image with echogenic inner rim and outer hypoechoic muscle layers (“double-halo” sign) is highly suggestive.
Colonic duplications can be cystic or tubular, the second being more frequent in the rectum.
If the cyst contains ectopic gastric mucosa or pancreatic tissue and communicates with the rectum, rectal bleeding may occur.
Fig. 2.126a, b Cystic duplication of the colon. (a) Sonography shows a round, fluid-filled image (C). Note the inner echogenic layer (arrowheads) and the outer hypoechoic rim (arrows). (b) CT scan of the same patient demonstrates a water-density cystic mass (C) surrounded by transverse colon gas (arrows).
Table 2.57 Intramural air in the gastrointestinal tract
Diagnosis
Findings
Comments
Pneumatosis intestinalis (small and large bowel; see Table 2.54)
Abdominal X-ray: linear or cystic (submucosal or subserosal) air in intestinal wall.
In NEC (perforation risk). May also occur in obstruction, Hirschsprung disease, cystic fibrosis, immunosuppression, etc.
Gastric pneumatosis
Linear or cystic lucencies in the gastric wall.
Tube malposition, after endoscopy, volvulus, ulcer disease, and from chemical damage.
Table 2.58 Calcifications and foreign bodies within the gastrointestinal tract
Small flecks of calcification in the lumen with meconium ileus and other congenital forms of obstruction.
Neonates.
Enterolith
Due to chronic fecal retention with anorectal anomalies. Begins as a soft-tissue density and later increased in density due to peripheral apposition of calcium salts.
Enterolith in a Meckel diverticulum
Rare.
Fig. 2.127 Appendicolith. An appendicolith is seen in this abdominal plain film adjacent to right L4 transverse process.Fig. 2.128 Appendicolith. Doppler US longitudinal scan shows several hyperechoic stones with acoustic shadowing inside the lumen of a dilated, inflamed appendix.
Only gold members can continue reading. Log In or Register to continue