Area of localized swelling with central crater, converging folds where there is scarring.
Clinical symptoms unreliable. Multiple ulcers are frequent. Endoscopy.
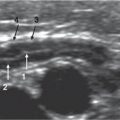
Benign polyps
Filling defects of variable size, single or multiple.
Mostly at the region of the duodenal bulb or at the inferior portion of the duodenal loop.
Differentiation is only possible histologically. Ectopic pancreas may be present. Malignant tumors have not been described in children.
Foreign bodies
UGI: may delineate a nonopaque foreign body.
Hair clips, peanuts, hot dogs, etc. Danger of perforation.
Erosive duodenitis
Filling defects with punctuate depressions.
Colicky abdominal pain.
Gastric, bulbar, and duodenal varices
Round, oval impressions in the bulb and/or duodenum; alteration with change in position on the contrast examination.
Portal hypertension.
Fig. 2.76 Duodenal ulcer. Two small ulcers (aphtha) with a central barium-filled hole and rounded peripheral edema are seen in the third duodenal portion in a patient with Crohn disease.Fig. 2.77 Duodenal ulcer. An additional image (arrowhead) is seen in the pyloric channel, with peripheral edema.
Table 2.42 Duodenal atresia and stenosis
Diagnosis
Findings
Comments
Duodenal atresia
X-ray: “double bubble” sign. Rarely require further radiologic investigation and most patients are taken directly to surgery.
Most frequent cause of complete duodenal obstruction. Sixty percent are premature.
X-ray: dilatation of the stomach and duodenum with a normal or diminished amount of air in the small bowel.
UGI series: necessary to differentiate between midgut volvulus and partial duodenal obstruction caused by a web or stenosis, etc.
US: to rule out midgut volvulus (“whirlpool” sign) and extraluminal causes (duplication cyst, etc.).
Causes of partial duodenal obstruction: duodenal web, Ladd bands, annular pancreas, midgut volvulus, preduodenal portal vein, duplication cyst, and superior mesenteric artery compression.
Traumatic duodenal hematoma
Intramural lesion narrowing the duodenal lumen.
Due to fall, for example, onto bicycle handlebars.
Postoperative changes
Narrowed caliber with proximal dilatation. Paucity of small-bowel air.
Disparity of bowel caliper after removing stenotic or atretic segment may remain after surgical repair.
Superior mesenteric artery compression
Lineal abrupt intermittent obstruction of the third duodenal portion depending on patient position.
Small angle between aorta and the mesentery artery in a thin patient (body cast). May be familial.
Fig. 2.78 Duodenal web. The classic “double-bubble” image is depicted, with distention of the stomach and the duodenum proximal to the stenotic area, located in the fourth portion. No distal air is seen in this film, which was taken 6 hours after birth.
Table 2.43 The duodenum: Diverticula and duplications
Contrast examinations: the duodenum compressed by intramural mass in the duodenal c-loop (“beak” sign). US: cystic image with echogenic inner rim and outer hypoechoic muscle layers (“double-halo” sign) is highly suggestive.
Usually noncommunicating and located along the first and second portion of the duodenum on the mesenteric side.
Clinically: Symptoms of obstruction. They may cause biliary obstruction and pancreatitis.
Fig. 2.79 Duodenal duplication. (a) UGI series: The C-shaped duodenum is widened by a rounded mass. The lumen is compressed, but contrast passage is not blocked. (b) US shows the cystic mass. The clue to the diagnosis is the layered appearance of the wall (“double-wall” sign). The content has a fluid-fluid level. (c) T2-weighted MRI shows the cystic mass with wall identical to the rest of the bowel (arrowheads).Fig. 2.80 Duodenal diverticulum. UGI series shows a diverticulum of the third portion.
Small Bowel
Table 2.44 Displacement or separation of loops of small bowel
Supine abdominal radiograph: generalized high density, central position of bowel loops, and separated bowel luminogram (differentiate from thickened bowel wall or increased content).
Masses and tumors
Usually focal displacement depending on tumor origin.
Due to generalized lymphadenopathy (leukemia, Hodgkin disease), mesenteric cysts, inflammatory masses in Crohn disease, ovarian tumors, small bowel exophytic tumors, etc.
Table 2.45 Diminished or absent air in the small bowel
Distal absent bowel air. DD with distal obstructions with bowel loops filled. Upright X-ray can show airfluid levels.
Congenital: esophageal atresia types I, II, and IIIa (no fistulous connection with the dilated esophagus), duodenal atresia, agastria, pyloric atresia.
Scaphoid abdomen.
Proximal Functional Obstruction
Neonates and infants
Absent or diminished air/content in the small and large bowel. Normal GI tract may be patent insuffiating air through a nasogastric tube.
Poor sucking and swallowing. Prematurity, perinatal brain anoxia, severe RDS, parenteral hyperalimentation, maternal medication (e.g., sedation during delivery).
All age groups
Frequent vomiting of any etiology, poor swallowing (consumption).
Plain X-ray: numerous dilated loops of bowel occupying the entire abdominal cavity.
Meconium may be noted in the distal ileal loops. Contrast enema is mandatory: the colon is normally placed but has an abnormally small caliber (functional microcolon) (DD with colonic atresia).
Fifty percent of small bowel atresias. Intraperitoneal calcifications, indicative of meconium peritonitis, are not uncommon in ileal atresia. Pneumoperitoneum contraindicates colon examination.
Congenital short gut
Shortened narrow caliper bowel.
Anomalous mesenteric position, possibly associated with malrotation.
US: hyperechoic intestinal content (DD with ileal atresia).
Contrast enema: microcolon with multiple small filling defects (meconium pellets).
Therapeutic enema (high osmolar, nonionic water-soluble agents are the best choice) to help the passage of the sticky meconium relieving obstruction and avoiding surgery.
Low intestinal obstruction produced by impaction of abnormal meconium in the distal ileum.
Almost always in cystic fibrosis. The diagnosis may be confirmed by finding an increased concentration of sodium chloride in sweat.
Abdominal X-ray: linear or punctate calcifications over the serosal surfaces of the abdominal viscera. Distended loops of the bowel with air-fluid levels may be present due to the underlying intestinal obstruction. Ascites may be present.
In utero perforation of fetal GI tract during the last 6 months of pregnancy.
If perforation is patent at birth, free air will be seen in the peritoneal cavity or trapped in a walled-offiloculus or pseudocyst.
Functional immaturity of the colon: meconium plug syndrome and small left colon syndrome
Low bowel obstruction.
Contrast enema: narrow (micro) descending colon. Diagnose and treat with contrast enemas.
Typically, there is clinical improvement after the enema.
Premature infants. Both entities are associated with dysmotility of the colon.
Causes: diabetic mothers, septicemia, hypothyroidism, and hypoglycemia.
DD: meconium ileus and Hirschsprung disease.
Functional ileus of prematurity
Bowel distention usually is less severe than in organic obstruction. Few air-fluid levels.
Temporary poor intestinal function during the first days of life (immaturity of the neural plexus).
Necrotizing enterocolitis (NEC)
Abdominal X-ray: gaseous distention and thickened bowel walls. Pneumatosis intestinalis (submucosal or subserosal air). May be linear (submucosal) or cystic collections (subserosal).
Portal vein gas: finely branching radiolucencies from the porta hepatis to the periphery of the liver.
Premature infants, within the first 2 weeks of life.
Fig. 2.81 Jejunal atresia. Supine radiograph shows a few dilated air-filled intestinal loops, about four “bubbles,” which indicates a high obstruction. No distal air is seen.Fig. 2.82a, b Ileal atresia. (a) Supine abdominal radiograph shows multiple dilated air-filled bowel loops occupying the entire abdominal cavity. With any degree of distention, it is impossible to differentiate the small bowel from the colon. (b) Contrast enema outlines the small size of the colon corresponding to an unused colon.Fig. 2.83 Meconium ileus. Water-soluble contrast enema shows a microcolon with scattered filling defects that correspond to inspissated meconium.Fig. 2.84a, b Meconium peritonitis. (a) Abdominal radiograph demonstrates a small amount of air in a markedly distended abdomen. A calcified mass within the peritoneal cavity is observed (arrows). There is no pneumoperitoneum. (b) Sonography of the same patient shows a pseudocyst containing debris with peripheral calcification.Fig. 2.85 Meconium peritonitis with calcified meconium in the scrotum. Plain radio-graph at birth shows scattered areas of calcification in the scrotum (arrowheads). Small flakes of intra-abdominal calcifications are also observed (arrows).
Table 2.47 Small-bowel distention: Infants, toddlers, and older children
Diagnosis
Findings
Comments
Prominent intestinal air
Slightly dilated bowel loops.
Caused by long bouts of crying in young children.
Distended stomach predominance.
Mechanical obstruction (SBO)
Disparity in size between obstructed proximal and distal bowel loops. Hyperactive peristalsis/aperistalsis (“fatigued” small bowel). Supine X-ray: progressive increase in luminal fluid/gas relation leads to sequential features: “stretch sign,” “stepladder appearance,” and “string of beads.”
In cases of fluid-filled intestine without air, SBO may be overlooked in supine X-ray films.
All age groups.
Complete SBO: colon empties in 12–24 h.
Supine X-ray has sensitivity of less than 50% in SBO.
Coiled-spring appearance on contrast exams. Cross-sectional methods: “crescent-in-doughnut” sign (axial images) and “sandwich” sign (longitudinal). Ileocecal valve not involved.
Usually transient, asymptomatic, mobile, and smaller (< 3 × 2 cm) than ileocolic intussesception. Frequent in sprue and enteritis. Consider surgery in cases with peritoneal trapped fluid, lead point (polyp, lymphoma, Meckel), obstruction, or when longer than 3.5 cm.
Edema and hemorrhage of the bowel wall with peritoneal fluid. If necrosis develops, gas may be present in the bowel wall, portal venous system, and in the peritoneal cavity (patent perforation). Supine X-ray: “coffee-bean” sign (gas-filled loop excluded) and “pseudotumor” sign (fluid-filled loop). “Whirl” sign (twisting of bowel and mesentery) on cross-sectional imaging.
Mechanical obstruction with interruption of arterial blood supply. Closed-loop obstruction: bowel obstruction at two points. Caused by: volvulus, incarcerated hernia, adherences, etc.
Adynamic-paralytic ileus
Generalized dilatation (including stomach and rectum) with normal folds and air-fluid levels. “Sentinel loop” if ileus is localized.
Malabsorption syndromes: Celiac disease (sprue) and lactase deficiency
Fluid distended loops of the small bowel (hypotonic) with normal fold thickness and some air-fluid levels due to secretions. See Table 2.48.
Sprue: Malabsorption due to gluten intolerance. Atrophy of folds. Intestinal biopsy confirmatory. Lactase deficiency: Addition to lactose to the barium contrast reproduces symptoms and malabsorptive findings.
Transient (electrolyte imbalance, renal or heart failure) or chronic idiopathic (females).
Fig. 2.86a, b Inguinal hernia. (a) Plain abdominal film shows bowel loops inside the right scrotum; a mild proximal bowel dilatation is seen. (b) Scrotal longitudinal US shows the scrotal hernia with ascitis and bowel loops inside the iguinal channel superior to the scrotal content.Fig. 2.87a–d Midgut volvulus. A 12-day-old girl with bilious vomiting. (a) Plain abdominal film with “double bubble” sign in a neonate with a complete duodenal obstruction. Note the dilated stomach and duodenum. (b) UGI series that shows the pathognomonic “corkscrew appearance” (arrows). (c) Transverse B-mode sonography of the upper abdomen shows the twisting of bowel, mesentery, and superior mesenteric vein around the axis of superior mesenteric artery (arrowhead). (d) Color Doppler image demonstrates a circle of vascularity that represents the superior mesenteric vein twisting around the superior mesenteric artery, producing the characteristic “whirlpool” sign.d duodenumst stomachFig. 2.88a–c Intestinal malrotation. (a) UGI series demonstrates the small intestine located in the right hemiabdomen and the colon in the left, corresponding to a nonrotation. (b) Transverse sonogram that shows the superior mesenteric vein lying to the left of the superior mesenteric artery. (c) Contrast-enhanced CT scan shows the same findings as an US. Note the superior mesenteric artery (black arrow) and superior mesenteric vein (white arrow).a superior mesenteric arteryv superior mesenteric veinFig. 2.89 Transient small bowel intussesception. US images: As an incidental finding in an asymptomatic patient, a transient intussesception is found. A small crescent-in-doughnut image (less than 2 cm) is seen in the transverse image (left). In the longitudinal scan (right), the intussesception is short with no lymphadenopathies inside. During the scan, peristalsis is seen inside the intussesception.Fig. 2.90 Ascariasis. Barium examination shows the ascaris worms as elongated tubular filling defects (arrows). The intestines of the worm are seen as stringlike white densities outlined by ingested barium (arrowheads).Fig. 2.91 Paralytic ileus. US image shows dilatation of small-bowel (left) and colon (right) loops in a patient with acute appendicitis.
Table 2.48 The small bowel: Diffuse parietal involvement
Usually thickened smooth folds, but occasionally irregular folds, scalloping, and thumbprinting may be seen.
Henoch-Schönlein purpura (nephritis, abdominal and joint pain) causes effacement small bowel wall layers (on US) and anechoic ascites. Often transient small-bowel IT and lymphadenopathy may be seen. Rarely affects the colon (DD hemolytic-uremic syndrome).
Hyperperistaltic intestine. Transient intussesception. Late stage: Thickened bowel wall with regular/irregular folds, depending of the infectious agent and the evolution stage. Rarely ascites.
Granular and linear ulcerations (cobblestone pattern), thickening of bowel wall with submucosal enlargement followed by loss of the stratification in fibrous rigid narrow segments. Fistulas, abscesses, fibrofatty proliferation of the mesentery, and lymphadenopathies separating the bowel loops.
Chronic idiopathic disease related to immunologic disorder in predisposed genetic patients, post GI infection in some cases. May affect any part of the GI tract, particularly the terminal ileum. Discontinuity (skip lesions), transmural and mesenteric involvement, ulceration, and fistula are characteristic.
Excessive fluid in dilated small bowel with no fold thickening, (except at the duodenojejunal area) with normal fold pattern in the ileum (“jejunization of the ileum”): reversal of the jejunoileal fold pattern. Transient intussesceptions.
Sprue: Malabsorption due to gluten intolerance. Atrophy of the intestinal villi and folds. Small bowel flaccid and poorly contracting. Some air-fluid levels. Intestinal biopsy confirmatory. Complication: diffuse intestinal lymphoma.
Lactase deficiency
Addition to lactose to the barium contrast reproduces symptoms and malabsorptive findings.
Hydrogen breath test.
Connective tissue diseases (rare)
Hypomotility and “hidebound” sign of the folds (close together) due to the wall atrophy.
Symptoms depend on the type of autoimmune disease.
Food allergy or food intolerance
Bowel loops separated by edema of the wall and mesentery. Hypersecretion.
Allergic (food intolerance type IV) or immunologic etiology. Eosinophilia. GI symptoms related to ingestion of specific foods. Self-limiting nature. Steroid therapy response.
Eosinophilic enteritis
Usually thickened irregular mucosal folds with jejunum predominance and concomitant gastric involvement. Rigidity, separation of the bowel loops, and hyperplastic lymph nodes may simulate Crohn disease.
Lymphangiectasia
Edematous regular thickening of small bowel mucosal folds (due to lymphatic dilatation and protein loss) with no evidence of liver, kidney, or heart disease is suggestive.
Primary or secondary (inflammatory or neoplastic lymph nodes) block lymphatic outflow.
Whipple disease
Duodenal and jejunal thickened irregular distorted folds.
Large hypoechoic/hypodense bulky lymphadenopathy in the mesentery and retroperitoneum is very characteristic.
Arthritis, fever, and lymphadenopathy may precede diarrhea. Macrophages and glycoprotein granules are positive for periodic acid–Schiffin the lamina propria. It is caused by Tropheryma whippleii, a Gram-positive bacilli. Revert to postantibiotic therapy.
Thickened mucosal folds in proximal jejunum associated with duodenal findings (thickened coarse fold pattern: nodular, poor defined folds, kinking, and distortion of duodenum).
Associate changes in the liver, bile ducts, and pancreas (see Tables 2.15and 2.17). Adherent collections of viscous mucus, hyperplastic appearance of the colon mucosa. Residual thick secretions.
Localized in a segment (75%) usually ileum, multifocal (polyp/stenosis) or diffuse (thick or obliterated folds). Exophytic and mesenteric masses. Aneurysmal dilatation (slough of the necrotic core of a large mass).
Primary or secondary.
Possible enlargement of mesenteric and retroperito-neal lymph nodes.
Alpha-beta-lipoproteinemia
Dilatation and moderate regular thickness of the small bowel.
Rare inherited malabsorption of fat, neurologic deterioration and retinitis pigmentosa.
Xanthomatosis
Regular thickness of the small bowel.
Multicentric proliferation of lipid-laden cells is initially a cutaneous disorder.
Irregular thickness of the small bowel due to the infiltration of inflammatory cells most apparent in the duodenum and jejunum. Hypermotility, secretions.
Acute gastroenteritis (GE), malabsorption syndrome associated with GI immunodeficiency syndrome. Characteristic cyst in the mucus (smear/bowel biopsies).
Other
Radiation injury. Mastocytosis. Mucositis.
Fig. 2.92 Bowel edema in portal hypertension. US image shows edema of small bowel (a) and colon (b). Note in (a) that mesenteric edema is also present (arrowheads).Fig. 2.93 Bowel hemorrhage in a patient with Henoch-Schönlein purpura. Doppler US shows vascularized, fluid-filled small-bowel loops with parietal thickening.Fig. 2.94a, b Intramural hematoma in a boy with hemophilia. (a) Sonogram (transverse section) of an ileum loop shows marked bowel wall thickening (arrow and arrowhead) with poorly defined wall stratification. (b) Unenhanced CT scan shows circumferential thickening in cross-section of ileal wall (arrow) with adjacent stranding of mesentery.Fig. 2.95a, b Giardiasis. (a) Barium small-bowel examination in a patient with immunoglobulin A deficiency demonstrates dilution of barium and an apparent fold thickening. (b) The same patient shows a fine nodular pattern at the terminal ileum.Fig. 2.96a–d Crohn disease. (a) Barium small-bowel examinations. (1) Aphtha (arrows) in the proximal jejunum with more advanced disease is found distally (not shown). (2) Transversely oriented linear ulcers (fissures) are a frequent finding in Crohn disease. (3) Many linear and transverse ulcerations separating islands of protruding mucosa are present and give rise to a cobblestone appearance. (b) Barium small-bowel examination shows extensive ulcerated Crohn disease with ulcers, thickened folds, strictured segments, pseudodiverticula, and mesenteric involvement. (c) True fast imaging with steady state precession MRI (coronal: left; axial: right) demonstrates bowel wall thickening at the distal ileum (arrows) and a slight distortion of the bowel folds. (d) Doppler sonogram demonstrates an increased flow in the affected intestinal segment.Fig. 2.97a–c Crohn disease of the terminal ileum. (a) US axial image shows transmural regular thickening with conspicuous submucosal layer. (b) In another area, with more advanced stage, the wall thickening is asymmetric with irregular mucosal surface due to ulcerations. The mesentery is also affected. (c) CT shows the ileocecal region with the valve rigid and open and parietal thickening both the caecum and the terminal ilium.Fig. 2.98a, b Celiac disease. (a) Barium small-bowel examination shows dilatation with hypersecretion and flocculation. There is an increase of normal fold pattern in the ileum (“jejunization of the ileum”) and their reduction in the jejunum (“moulage” sign). Hypomotility was demonstrated fluoroscopically. (b) Barium examination shows severe flocculation and segmentation of the barium as a consequence of a very slow transit.Fig. 2.99 Cystic fibrosis. Longitudinal US of the appendix shows dilatation of lumen due to inspissated mucus and feces. The incidentally increased diameter of the appendix (> 6 mm) must not be interpreted as a sign of acute appendicitis.Fig. 2.100 Small bowel Burkitt lymphoma. Longitudinal Doppler US scan shows a pseudokidney image cranial to the bladder.Fig. 2.101a, b Small bowel non-Hodgkin lymphoma with intussusception. (a) Longitudinal image in the right flank shows an ileocolic intussesception with a hypoechoic mass at the apex (arrowhead), located in the subhepatic area. (b) Hypervascular lymph nodes are seen in the mesogastric area in the Doppler US image.
Table 2.49 The small bowel: Focal parietal involvement and filling defects (solitary)
Multiple coarse, nodular outline of the lumen; wall infiltration with long segment narrowing of the lumen; polypoid form has a tendency to intussesception; endoenteric and exoenteric types with crater and fistula formation; tumor infiltration in the mesentery with a spruelike appearance.
Depicted accurately on cross-sectional imaging techniques.
Carcinoid
Parietal ileal small lesion with desmoplastic response (kinking and rigidity of the bowel, mesentery, and vessels).
Elevated 5-indolacetic acid. Scintigraphy with (123) I-MIBG is diagnostic.
Table 2.50 The small bowel: Multifocal parietal involvement and filling defects (multiple)
Peutz–Jeghers syndrome (hamartomatous): Hereditary. Oral and perioral pigmentosus. Intussusception. Anemia. Most frequent in the jejunum.
Juvenile polyposis: predominantly colonic.
Multiple simple adenomatous polyps.
Gardner syndrome: diagnosis based on histology.
Hemangiomatosis
In Rendu-Osler syndrome.
Lymphangioma
US and MRI are diagnostic.
Malignant tumors
Lymphoma. Metastatic Wilms tumor (rare, filling defects impinges on the bowel lumen); intussesception.
Table 2.51 The small bowel: Diverticula and duplications
Diagnosis
Findings
Comments
Meckel diverticulum
Contrast demonstration of the diverticulum is rarely accomplished. May produce intussesception, obstruction, diverticulitis, and enterolith formation.
Remnant of the omphalomesenteric duct in the antimesenteric side. Ectopic gastric mucosa present in 30% of cases may cause hemorrhage (positive scintigraphy).
Duplications (enteric cysts, neurenteric cysts)
Barium examination: compression may produce a “beak” sign.
On the mesenteric side US: a cystic image with echogenic inner rim and outer hypoechoic muscle layers (“double halo” sign) is highly suggestive of duplication.
DD: choledochal cyst, pancreatic pseudocyst, and mesenteric cysts.
Most common location is the ileum, followed by the duodenum.
May be cystic or tubular, the second being more frequent in the rectum.
A cyst located in the ileum at the ileocecal junction can manifest as an intussesception.
Diverticulum
On the antimesenteric side.
Complication: infection, ulceration, and perforation.
Only gold members can continue reading. Log In or Register to continue