US: best imaging screen method. US findings: elongation of the pyloric channel (≥ 16 mm).
Persistent thickening of the pyloric muscle (> 3 mm) in the elongated portion of the canal.
Hypoechoic “doughnut” (thickened muscle) on axial projection.
Vigorous peristalsis.
Gastric outlet obstruction leads to emaciation. “Projectile” vomiting.
DD: congenital pyloric stenosis, “prostaglandin E induced stenosis outlet”: the stenosis is produced by central foveolar hyperplasia. Mucosal changes are different from the muscular thickening observed in HPS.
Roviralta syndrome: HPS and hiatal hernia.
Pylorospasm
US: Persistent spasm of the pyloric canal with little fluid passing into duodenum. Bo rderline measurements. No evidence of hyperperistalsis.
Typically intermittent. Serial US useful to differentiate from hypertrophic pyloric stenosis (HPS).
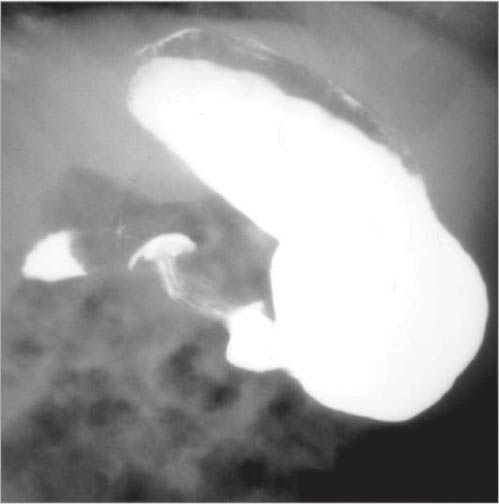
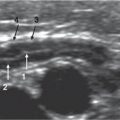
Fig. 2.60 Tracheal tube malposition. Chest X-ray in a newborn with neonatal respiratory distress. The endotracheal tube is malpositioned inside the esophageal lumen. Note that the tracheal lumen (arrowheads) is located anterior to the nasogastric and tracheal tubes.Fig. 2.61 Hypertrophic pyloric stenosis. UGI series of a newborn with persistent vomiting shows gastric distension with emptying diff culty throughout an elongated pyloric channel with “double channel” image.Fig. 2.62 Hypertrophic pyloric stenosis. US images of pylorus in a 21-day-old boy with persistent vomiting. In the longitudinal image (left), the pyloric channel is elongated and the muscular layer is hypoechoic and thickened. Axial scan (right) shows a doughnut image in the subhepatic region with a double pyloric channel image produced by folding of the hyperechoic mucosal surface. No passage of gastric content is observed during the exploration period.Fig. 2.63 Pyloric atresia. Anteroposterior plain abdominal radio-graph in a newborn with pyloric atresia that shows distention of the stomach (st) and absence of air in the small bowel and colon, resulting in the characteristic “single bubble” image.Fig. 2.64 Antral web. UGI series shows an incomplete antral web. In this oblique view, a concentric radiolucent band (arrows) is seen, resulting in discrete antral lumen reduction. The arrowhead indicates where the pylorus is located.
Mucosal Changes
Table 2.37 The stomach: Mucosal changes and filling defects
Diagnosis
Findings
Comments
Inflammatory Changes
Infectious gastritis
Helicobacter pylori: enlarged gastric folds in the body and antropyloric regions of the stomach.
Cytomegalovirus (CMV): often causes deep ulcerations, submucosal masses resulting from edema, or local microabscesses.
Helicobacter pylori has been related to gastritis and peptic ulcer. Associated with AIDS, CMV, Toxoplasma gondii, Cryptosporidium, or human immunodeficiency virus direct damage.
Caustic injury (chemical gastritis)
Plain radiographs: always, to assess perforation. Double-contrast exam: in absence of perforation (if perforation exists, water-soluble contrast materials are mandatory). Severe mucosal edema and spasm and narrowing of the stomach are the most common findings.
Alkali is the most common substance. Despite it usually causing esophagitis, antral and pyloric channel gastritis is found in up to 20% of cases.
UGI exam: marked enlargement of the fundal rugae, commonly along the greater curvature.
US: Thickening of the gastric mucosal folds if examination is performed with an empty stomach. In a fully filled stomach, hypertrophied rugae collapse. Thickening occurs on the submucosal layer of the stomach.
Uncommon self-limited disease. Cause unknown (hypersensitivity response and viral infection have been reported).
Nausea and vomiting in association to protein-loss enteropathy. Pleural effusion, ascites, and peripheral edema.
Ulcer disease
Ulcer crater usually associated with thickening mucosal folds (superficial in stress ulcer and drug erosive gastritis).
Barium examination, US, CT, and MRI: Intramural masses in all sort of sizes. Occasionally might be multilobar and show an exophytic growing.
Less well-differentiated stromal tumors of the GI tract.
Carcinoma
Varied appearances.
CT: very useful to demonstrate the extragastric component of the tumor.
Anomalies
Microgastria
The shape of the stomach is tubular or saccular, small in size, usually nonrotated, and in some cases located partially in the intrathoracic space. Almost all cases are associated with severe GER and a dilated lower esophagus.
Barium examination: Small (1–3 cm) broad-based submucosal mass on the larger curvature. At times, central umbilication (rudimentary pancreatic duct). Can easily be misinterpreted as a gastric submucosal tumor.
Pancreatic tissue that lacks anatomic and vascular continuity with the main body of the pancreas. Most common location: gastric antrum.
May prolapse into the pylorus, producing intermittent obstruction.
Plain X-ray: intragastric mass with solid or bizarre appearance, frequently rounded by air.
Barium exams: contrast may either soak or superficially coat the mass.
US: hyperechoic line with progressive sound attenuation.
Trichobezoars: swallowed hair. In adolescence. Phytobezoars: vegetal matter (coconut, raw oranges).
Lactobezoars: incorrectly prepared powdered milk formula (highly concentrated).
Prolapsed gastric mucosa
Filling defects in duodenal bulb.
Gastric (fundal) varices
GI series: serpiginous filling defects in antrum and lesser curvature.
Associated with esophageal varices in patients with portal hypertension. More common in splenic vein thrombosis.
Hematoma/hemorrhage
Thickened mucosal folds.
Trauma, child abuse, hemophilia.
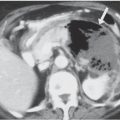
Fig. 2.65 Ménétrier disease. UGI series shows rugal hypertrophy in a 5-year-old boy with hypoproteinemia and Ménétrier diseaseFig. 2.66 Chronic granulomatous disease. UGI series depicts a tapered antral stenosis with benign appearance in a 9-year-old boy with chronic granulomatous disease. Contrast retention in the stomach is also noted.Fig. 2.67 Leiomyoblastoma. UGI series depicts a filling defect in the antral region (arrowheads) produced by a submucosal tumor (leiomyoblastoma).Fig. 2.68 Non-Hodgkin lymphoma. US transverse scan of the stomach in a 5-year-old girl shows a narrow hyperechoic mucosal lumen (arrowheads) and a thickened, tumoral infiltrated wall, depicted as a rounded hypoechoic mass (M).Fig. 2.69 Burkitt lymphoma and gastric involvement. CT scan of a 7-year-old boy: note the existence of a small homogeneous, polypoid, rounded mass located in the posterior fundic wall (arrow).Fig. 2.70a, b Gastrointestinal stromal tumor. (a) US performed with the stomach lumen fully filled with water (L). A solid, mostly hypoechoic, submucosal mass (M) is depicted. Note that the mucosal layer (m) is patent and unaffected. (b) Axial CT with intravenous contrast in the same patient. Note that the mass (M) is not enhancing despite the intravenous contrast administration.Fig. 2.71 Ectopic pancreas. A left-posterior oblique view of a UGI series performed in a 7-year-old boy: The ectopic pancreatic tissue measures less than 2 cm in size and is classically located within 6 cm from the pylorus in the gastric antrum (arrow). The presence of ulceration could not be assessed in this study despite the clinical diagnosis of microcitic anemia.Fig. 2.72 Large gastric trichobezoar. A 13-year-old girl with abdominal pain: plain abdominal film shows a distended air-filled stomach with a large intraluminal mass outlined by air.
Table 2.38 The stomach: Diverticula and duplications
Diagnosis
Findings
Comments
Diverticulum
Barium exam: round or oval pouch with a small neck that typically changes in shape and size.
Uncommon in any age group. Represent communicating duplications.
Usually in the cardiofundal and antropyloric regions.
US: well-defined cystic mass lying close to the greater curvature of the stomach. The presence of an echo-genic inner rim and hypoechoic outer muscle layers is highly suggestive.
CT: sharply marginated, with a homogeneous near-water density, not enhancing after intravenous contrast material injection.
MRI: low signal intensity on T1-weighted images and high signal intensity on T2-weighted images.
Seven percent of GI tract duplications.
Fig. 2.73a–d Gastric duplication cyst. (a, b) UGI contrast study outlines an intra-abdominal mass displacing the stomach and bowel up and to the right. (c) US scan through the gastric body shows a cystic mass with no communication with the gastric lumen and with a double-layered wall (landmark of duplication). (d) Sagittal T2-weighted MRI shows a cystic mass compressing the stomach wall.
Table 2.39 Alteration in gastric shape and position
Diagnosis
Findings
Comments
Cascade stomach
Fundus folded posteriorly that empties into the antrum (horizontal stomach).
Caused by overdistention of transverse colon, splenomegaly, tumors, etc.
Dilated stomach. Mesenteroaxial volvulus: the cardia is inferiorly displaced and the pylorus is in a higher subdiaphragmatic position.
Organoaxial volvulus: greater curvature to the right of the lesser one.
Mesenteroaxial volvulus: Associated with left hemidiaphragm elevation. Associated with big hiatal hernias, particularly paraesophageal.
Organoaxial volvulus asymptomatic in neonates.
Fig. 2.74 Organoaxial volvulus. A 3-month-old boy with persistent vomiting: UGI series shows the greater curvature located to the right and superior to the lesser curvature. The twisting is only of 180 degrees, thus permitting the passing of oral contrast.
Only gold members can continue reading. Log In or Register to continue