|

Identify the normal anatomy of the liver including the liver lobes, segments, fissures, ligaments, and hepatic vasculature.
Describe the different lobar divisions of the liver including anatomic, functional, and Couinaud’s segmental divisions.
List some of the various functions of the liver.
Discuss the laboratory values associated with liver function.
Explain the patient preparation, scanning technique, and sonographic appearance of the normal liver.
Discuss the pathophysiology and sonographic appearance of diffuse liver diseases including fatty infiltration, hepatitis, and cirrhosis.
Describe the differential diagnoses, clinical signs, symptoms and sonographic appearance of cystic and solid liver lesions.
Discuss ultrasound contrast enhancement of the liver, when to use it, and how it helps with diagnosing solid masses.
Discuss the benefits of elastography of the liver.
more echogenic than the liver in a patient with hepatitis, whose inflamed liver is abnormally hypoechoic.
 FIGURE 7-1 Fetal circulation. The umbilical vein carries oxygenated blood from the placenta to the fetus, ascends the fetal abdomen, and courses toward the liver. A portion of blood flow is allowed to bypass the fetal liver via the ductus venosus. After birth, both veins close and exist as ligaments; the umbilical vein becomes the ligamentum teres and ductus venosus becomes the ligamentum venosum. |
from 13 to 15.5 cm, although some references go as high as 17 cm.11 An AP measurement can be obtained on the same image as the length if needed. The length of the liver is obtained by measuring the liver from the diaphragm to the tip of the RL at the right midclavicular level, which is an imaginary vertical line that goes through the middle of the clavicle.10,11 The liver’s size can increase with increased height and body surface area and decrease with age.10 Liver length is needed to determine if hepatomegaly is present.
 FIGURE 7-2 Liver location. A: The liver occupies the right hypochondrium, the greater part of the epigastric region, and extends in varying degrees into the left hypochondrium as far as the mammary line.3 The lateral segment of the left lobe and the length of the right lobe determine the contour and shape of the liver. Overall, the liver can be described as irregular, hemispheric,2 or wedge-shaped.3 B: The relationship of the liver to surrounding anatomy is illustrated in a lateral, sagittal section. |
 FIGURE 7-3 Normal sonographic anatomy. A: sagittal image of the right lobe (RL) of the liver demonstrating the normal increased echogenicity relationship between the normal liver and normal right kidney (RK). B: A transverse image demonstrating the normal homogeneous echo pattern of the liver and the three main hepatic veins, the right hepatic vein (RHV), the middle hepatic vein (MHV), the left hepatic vein (LHV), and the inferior vena cava (IVC). |
layer of connective tissue that covers the entire liver and each lobule. Glisson capsule contains blood, lymphatic vessels, and nerves and is highly echogenic by sonography.10,13,14 Distention of the capsule from liver disease or swelling can cause pain, and lymphatics may ooze fluid into the peritoneal space.13 Glisson capsule also ensheaths the portal triad, which consists of a branch of the hepatic artery, portal vein, and bile duct, which explains why the portal triad has echogenic borders.
 FIGURE 7-4 Normal anatomy. A: Anterior surface. The ligamentum teres begins at the umbilicus and courses within the falciform ligament to a deep notch called the umbilical notch, which is located on the anterior surface of the liver. The falciform ligament divides the liver into right and left anatomical lobes and will become the coronary ligaments. Opposite the cartilage of the ninth rib is the fossa for the gallbladder fundus.9 B: Posterior surface. The posterior portion of the liver is round and broad on the right and narrow on the left.3 The caudate lobe lies between the inferior vena cava (IVC) and the ligament venosum, which is not marked on this image.3,9 The posterior surface is in direct contact with the diaphragm and is attached by loose connective tissue. Most of the liver is covered by peritoneum except for the bed of the gall bladder, the porta hepatis, and where the liver is in direct contact with the diaphragm called the bare area. The bare area is bounded by the superior and inferior reflections of the coronary ligament, which connect the liver to the diaphragm.9 C: Posterior inferior view of visceral area: The right subphrenic space is seen between the right lobe of the liver and the inferior surface of the diaphragm. The left subphrenic space is seen between the diaphragm and the spleen. From lateral to medial, the right lobe has three impressions—the colic impression, which is a flattened or shallow area for the hepatic flexure; more posterior is the larger and deeper impression for the right kidney; and lying along the neck of the gallbladder, the duodenal impression is a narrow, poorly marked area.3 On the left, the gastric impression for the ventral surface of the stomach is a large, hollow area extending to the liver margin. D: Visceral surface. The visceral surface is concave and faces posterior, caudal, and to the left.3,9 The caudate process is just anterior to the IVC and connects the caudate lobe to the right lobe.9 On this image, the ligamentum venosum is seen with the caudate lobe located between the ligamentum venosum and the IVC. The portal triad as it enters the liver via the porta hepatis is illustrated. |
porta hepatis, and the IVC groove. It is in contact with the esophagus, the stomach including the pylorus, the first part of the duodenum, the right hepatic flexure, the transverse colon, the lesser omentum, the gallbladder, the right kidney, and the right adrenal gland.
TABLE 7-1 Ligament Attachments to the Liver | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
surface.16 It is somewhat quadrilateral. The posterior surface is marked by three fossae: the porta hepatis, the gallbladder, and the IVC.17
 FIGURE 7-5 Ligaments. A: The gastrohepatic ligament originates on the undersurface of the liver and courses caudal to attach to the lesser curvature of the stomach and the first portion of the duodenum. The hepatoduodenal ligament is located on the right free edge of the gastrohepatic ligament, surrounds the portal triad, and forms the anterior boundary of the epiploic foramen or the foramen of Winslow. B: Enlarged cutaway view of the hepatoduodenal ligament showing the portal triad. |
 FIGURE 7-6 Anatomic division. The “H” configuration on the visceral surface of the liver is as follows: An imaginary line from the gallbladder fossa to the inferior vena cava (IVC) fossa makes the right vertical limb. This separates the right lobe from the caudate and quadrate lobes. The left vertical limb is a line created by the falciform ligament and the ligamentum venosum and separates the left lobe from the caudate and quadrate lobes.9. The transverse limb is the porta hepatitis and separates the caudate and quadrate lobes. The gallbladder fossa is shallow and oblong, extending from the inferior margin to the right border of the porta hepatis.9 The IVC fossa is a short, deep depression between the caudate lobe and the right lobe. |
veins, and the ligamentum venosum and ligamentum teres (Fig. 7-7A). The lobes and segments are the RL, with an anterior and a posterior segment, the left lobe, with a medial and a lateral segment, and the CL.15 A combination of scanning planes that includes transverse, oblique, and parasagittal is needed to delineate the landmarks to identify the lobes and segments.
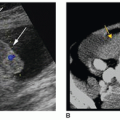
high posterior hepatodiaphragmatic interposition of the colon, and situs inversus (Fig. 7-9A-C).9,20,25 A common variant that can mimic hepatomegaly is called a Riedel lobe, which is a downward projection of the RL. (Note that the proper name is Riedel lobe and not Riedel lobe.) It is more common in women than in men. Sonographically, a Riedel lobe is identified as a finger-like or a tongue-like projection of the RL that extends past the ribs and may reach as far as the iliac crest25 (Fig. 7-10A, B). A Riedel lobe can be felt clinically, and the patient may be referred for a liver ultrasound to rule out a liver mass or hepatomegaly. To differentiate it from a mass, the sonographer must observe consistency of the echotexture between the Riedel lobe and the rest of the RL. To differentiate it from hepatomegaly, the sonographer should note that the rest of the liver’s size appears normal, and that the lobe comes to a point, whereas with hepatomegaly, the lobe has a more rounded edge (also see Fig. 7-16F, G). In hepatomegaly, the RL of the liver can displace the right kidney downward and up toward the diaphragm whereas a Riedel lobe “skims” across the top of the kidney.
 FIGURE 7-7 Segmental division. A: A “see-through” anterior to posterior profile. The dotted lines will be referenced in subsequent illustrations and sonograms. Segmental anatomy. B: An illustration through vertical plane B (Fig. 7-7A), which represents the main lobar fissure, which is seen sonographically between the gallbladder neck and the RPV and is used to divide the liver into its segmental right and left lobes. C: A parasagittal scan displays a portion of the MLF, seen as a linear echogenic line extending from the RPV to the GB separating the RL from the LL. D: An illustration through vertical plane C (Fig. 7-7A), the right intersegmental fissure, where the RHV courses between the right anterior and right posterior branches of the portal vein. E: A parasagittal scan through the RHV, which is the sonographic landmark dividing the right lobe of the liver into anterior and posterior segments. F: A transverse scan through the RHV dividing the liver into ASRL and PSRL. |
 FIGURE 7-7 (continued) G: An illustration through vertical plane A (Fig. 7-7A), the left intersegmental fissure, where the LHV divides the left lobe into lateral and medial segments. H: A parasagittal scan through the LHV and IVC. The caudate lobe is seen between the IVC and the LV. I: A transverse scan through the LHV dividing the left lobe of the liver into medial and lateral segments. J: LT (small arrows) is seen in the left lobe of the liver in the transverse plane as a rounded echogenic structure with an acoustic shadow. It serves as a landmark separating the MSLL and the LSLL of the left lobe. The LT should not be mistaken for a liver lesion. K: On this transverse image of a patient with cirrhosis and ascites, the falciform ligament (arrow) can be identified coursing between the anterior abdominal wall and the LLL which is very nodular. L: A transverse scan demonstrates the hepatic veins and liver segments. The MHV separates the right and left liver lobes. The LHV separates the MSLL from the LSLL. The RHV divides the ASRL from the PSRL. |
 FIGURE 7-7 (continued) M: A transverse image demonstrates the division of the RPV into anterior (ANT) and posterior (POST) branches. N: A transverse image demonstrates the division of the LPV into medial and lateral branches. O: A sagittal scan demonstrates the LSLL, which is delineated from the CL by a linear echogenic line representing the LV (arrow). P: The anatomy identified on this transverse scan includes the LSLL, which is delineated from the CL by the LV (arrow). Q: A parasagittal image demonstrates a small vein (arrows) draining directly from the CL into the IVC. ASRL, anterior segment of the right lobe; CL, caudate lobe; GB, gallbladder; IVC, inferior vena cava; LHV, left hepatic vein; LL, left lobe; LLL, left lobe of the liver; LPV, left portal vein; LSLL, lateral segment of the left lobe; LV, ligamentum venosum; LT, ligamentum teres; MHV, middle hepatic vein; MLF, main lobar fissure; MPV, main portal vein; MSLL, medial segment left lobe; PSRL, posterior segment right lobe; RAPV, right anterior portal vein; RL, right lobe; RHV, right hepatic vein; RPV, right portal vein. |
| ||||||||||||
supply the right anterior and right posterior intrahepatic lobar segments (Fig. 7-11K-N).9 The RPV divides into an anterior branch that supplies blood to segments 5 and 8, and a posterior branch that supplies blood to segments 6 and 7. Segment 1, the CL, is not considered to be part of either the right or left lobe and receives blood from multiple branches from both the left and right portal veins. The hepatic artery, portal vein, and intrahepatic duct course parallel to each other with hepatic and portal blood flowing into the liver and bile flowing in the opposite direction out of the liver (Fig. 7-11O). Intrahepatic ducts are not visualized routinely. If biliary radicles and portal venous radicles are imaged simultaneously side by side, the appearance, referred to as the parallel-channel sign, is used to diagnose biliary obstruction (Fig. 7-11P). Color or power Doppler imaging can distinguish the vessel from the bile duct. The biliary system is discussed in more detail in a later chapter.
 FIGURE 7-8 Couinaud’s anatomy. A: An illustration of the eight segments and how they are identified in a clockwise fashion. The hepatic veins divide the liver vertically into four segments and the portal veins divide the liver horizontally creating eight segments. The caudate lobe is segment 1 and is seen on the posterior aspect of the liver, it is not seen in an anterior view. B: A cross-sectional illustration high in the liver at the level of the hepatic veins identifies the four superior segments in Couinaud’s anatomy (PS = segment 7, AS = segment 8, MS = segment 4a, and LS = segment 2). C: A cross-sectional illustration at a midlevel through the liver identifies the right and left portal vein branches that correspond with the horizontal boundary. D: A cross-sectional illustration low in the liver at the level of the gallbladder and ligamentum teres identifies the four inferior segments in Couinaud’s anatomy (PS = segment 6, AS = segment 5, MS = segment 4b, and LS = segment 3). E: A transverse scan at the level of the hepatic veins demonstrates the superior segments. F: A transverse scan through the gallbladder and ligamentum teres demonstrates the inferior segments. |
| ||||||||||||||||||||||||||
 FIGURE 7-9 Situs inversus. A: Transverse scan on a newborn at midline demonstrating the liver in the left upper quadrant. B: Color Doppler image showing the inferior vena cava (IVC) on the left side of the abdomen and the aorta (Ao) on the right side. C: Parasagittal scan on the left side showing the right lobe of the liver and the right kidney. |
 FIGURE 7-10 A: An image of a Riedel lobe on a 36-year-old woman demonstrating this normal variant as an extension of liver tissue past the right kidney. B: Another example of a patient with a Riedel lobe and the liver measured 21.5 cm. |
 FIGURE 7-11 Vascular anatomy of the liver. A: Intrahepatic distribution of the hepatic arteries, hepatic veins, portal veins, and biliary ducts. An accessory or inferior right hepatic vein is illustrated draining directly into the IVC and is a variant identified in some patients. B: The vessels and ducts of the upper abdomen. C: A recumbent view of the relationship between the vessels and ducts of the upper abdomen. |
 FIGURE 7-11 (continued) D: A sagittal scan of the abdominal aorta (Ao), the celiac axis (CA), and the SMA. The celiac artery will curve back toward the liver while the SMA will run parallel to the aorta. E: A transverse midline scan images the CHA and SA as they come off of the CA. This appearance of CA, CHA, and SA is called the tail of a whale sign. The third branch of the CA, the LGA, is not seen. F: Color Doppler image of the CA and the CHA and SA. Because of the curviness of the vessels at times flow is going away from the transducer, blue signals, and then toward the transducer, red signals. G: A three-dimensional power Doppler image with grayscale subtraction displays the CA branching into the SA, CHA, and the least often detected third branch, the LGA. H: A lateral view of the same 3D data set offering better visualization of the LGA. |
 FIGURE 7-11 (continued) I: On this transverse image, the MPV can be seen entering the liver. J: This transverse scan demonstrates the LPV dividing into its medial and lateral branches. K: A transverse color Doppler image shows the RPV dividing into the anterior (ANT) and posterior (POST) branches. The posterior branch will be flowing away from the transducer toward the posterior aspect of the liver and blue is the correct color. L: An oblique view with color Doppler imaging the RPV and the LPV as they bifurcate demonstrating flow away from the transducer (blue) in the RPV branch and flow toward the transducer (red) in the LPV branch. IVC, inferior vena cava. M: A 3D reconstruction of the vessels at the porta hepatis with grayscale subtraction reveals the MPV, RPV, LPV, HA, and HV. |
 FIGURE 7-11 (continued) N: A side-by-side image of the portal vein with color Doppler image on the left and microflow imaging on the right demonstrating the branches coming off of the portal vein, which are not seen with conventional Doppler. With microflow imaging, slower flow and smaller vessels can be detected with better spatial resolution and improved sensitivity. O: An image showing the relationship of the CBD with the PV and HA. Both the CBD and HA should be anterior to the PV. P: The grayscale image on the left shows multiple tubular structures called the parallel-channel sign. The color Doppler image on the right shows that the parallel-channel sign represents dilated bile ducts, structures void of color, and normal portal veins, vessels with color. Q: The RHV, MHV, and LHV are seen in this transverse scan draining into the IVC. Transducer placement is at the sternum angling toward the patient’s head. R: On this transverse color Doppler image, all three hepatic veins are seen with hepatofugal flow, which represents flow exiting the liver as they drain into the IVC. S: A transverse oblique image through the right lobe demonstrating an ARHV and the RHV draining into the IVC. The middle and left hepatic veins are not seen in this image. Ao, aorta; ARHV, accessory or inferior right hepatic vein; CA, celiac artery; CBD, common bile duct; CHA, common hepatic artery; GB, gallbladder; GDA, gastroduodenal artery; HA, hepatic artery; HV, hepatic vein; IMV, inferior mesenteric vein; IRHV, inferior right hepatic vein; IVC, inferior vena cava; LGA, left gastric artery; LHV, left hepatic vein; LPV, left portal vein; LRA, left renal artery; LRV, left renal vein; MHV, middle hepatic vein; MPV, main portal vein; PHA, proper hepatic artery; PV, portal vein; RHV, right hepatic vein; RPV, right portal vein; RRA, right renal artery; RRV, right renal vein; SA, splenic artery; SMA, superior mesenteric artery; SMV, superior mesenteric vein; SV, splenic vein. |
Only pulsations should be exhibited by an artery or a vein.
An artery can indent the wall of a duct or a vein, but the reverse is not true. This is probably because of the lower venous and ductal pressures and the thicker, less easily deformed arterial wall.
The duct can occasionally decrease several millimeters in caliber during an examination and can have various calibers along its course, whereas arteries are uniform in caliber.
The artery may not parallel the portal vein or may do so only for a short distance, whereas the duct parallels the portal vein closely.
Arteries may be tortuous and loop in and out of the scanning plane.
Arteries produce pulsatile Doppler signals, veins produce continuous Doppler signals, and ducts produce no signal.
 FIGURE 7-12 A: Transverse section demonstrating the splenic vein (SV) and portal-splenic confluence (PSC). Locating the confluence at the level of the pancreas helps identify the origin of the main portal vein (MPV). B: An image of a portal triad showing the hidden “Mickey Mouse” sign. The MPV represents the face; the bile duct (BD) the right ear; and the hepatic artery (HA) the left ear. C: A color Doppler image of the hidden “Mickey Mouse” sign showing flow in the MPV and HA and no flow in the BD. Ao, aorta; SMA, superior mesenteric artery. |
 FIGURE 7-13 Microscopic anatomy. A: An enlarged sectional cut of the liver shows the hexagonal shape of its lobules. Each lobule measures several millimeters in length and 0.8 to 2 mm in diameter.4,9 B: The arrows indicate the direction of blood flow on this representation of one liver lobule. Constructed around a central hepatic vein, each lobule is composed principally of many cellular plates, or hepatocytes, the functional cells of the liver. The cellular plates radiate centrifugally from the central hepatic vein like wheel spokes.4 Hepatocytes are capable of regenerating, which allows damaged or resected liver tissue to regrow.13 A lobule has six corners. At each corner is a portal triad, so named because three basic structures are always present: a branch of the hepatic artery, a branch of the portal vein, and a bile duct.6,7 C: An enlarged schematic view of a small portion of one liver lobule illustrates the sinusoids and portal triad. Sinusoids are small capillaries that have a highly permeable endothelial lining located between the cellular plates. The sinusoids receive a mixture of portal venous and hepatic arterial blood.4,13 The blood drains into the central hepatic vein in the middle of each lobule and flows into the interlobular hepatic veins.4,13 Unlike other capillaries, sinusoids are also lined with phagocytic cells known as Kupffer cells.5,6,13 Kupffer cells belong to the reticuloendothelial system and function to remove foreign substances, such as bacteria and depleted white and red blood cells, from the blood.5,6 The Disse space, located between the endothelial lining and the hepatocyte, drains interstitial fluid into the hepatic lymph system.4,13 Small bile canaliculi are adjacent to the cellular plates and receive the bile produced by the hepatocytes.4,13 |
| ||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


