Fibromatosis colli
Fig. 4.163a, b |
US: Focal mass in or diffuse enlargement of the middle/lower third of affected SCM muscle. Variable echogenicity.
CT: enlarged muscle without discrete mass.
MRI: Usually iso-/hypointense to normal muscle on T1. T2 variable but usually hypointense at area of maximal enlargement probably due to fibrosis. |
Infant with torticollis tilting head to same side and rotating head toward opposite side. |
Lymph nodes/lymphoma
Fig. 4.164 |
US: Oval nodes increased in size and number. Central hypoechogenicity in suppuration.
CECT: best to differentiate cellulitis/phlegmon/abscess and assess extent of disease in suspected malignancy.
MRI: T1 low/intermediate signal; T2 high signal. |
Findings nonspecific and depend on clinical scenario; often rely on tissue diagnosis. |
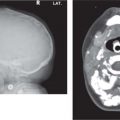
Teratoma
Fig. 4.130, p. 378 |
CT/MRI: Large and infiltrative with multiple cystic and solid elements. Contain fat and calcification. Both modalities show extent and components. |
Usually < 1 y; may cause significant airway and feeding compromise. |
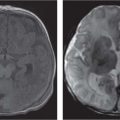
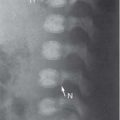
Neuroblastoma |
CT/MRI: Well-defined mass lying posterior to the vascular sheath and occasionally extending into the cervical spinal canal. MRI is best for delineating extent of tumor and spinal and intracranial extent. |
Less than 5% occur in the neck.
Need chest and abdomen CT as part of initial work-up to rule out abdominal primary. |
Hemangioma |
US: well-defined mass with prominent vessels.
MRI: Best for extent. T1 isointense to muscle with intense enhancement postcontrast; T2 hyperintense with multiple flow voids. |
Characteristic presentation; therefore, imaging indicated if suspect deep extension, pretreatment, or to assess treatment response. |
Rhabdomyosarcoma |
CT: heterogeneous lesion with or without osseous destruction.
MRI: isointense to muscle on T1, hyperintense on T2 and show enhancement postcontrast. |
May be a primary lesion or related to metastatic adenopathy that is present in 50% of patients.
Forty percent occur in head and neck. |
Fibrosarcoma/sarcoma |
CT/MRI: Heterogeneously enhancing soft-tissue mass. Usually less intense and homogeneous enhancement than hemangioma. May show osseous destruction. |
Often with regional lymph node involvement. Need chest CT for metastatic surveillance. |
Hematoma |
US: Imaging findings depend on age of bleed. Acute bleed hyper-echoic, less echogenic in 96 h, and eventually anechoic. Usually well defined but may become irregular if blood escapes into adjacent structures. Differentiate from tumor by absence of flow. |
Usually due to trauma, anticoagulation, or coagulopathy. |
Neurofibroma/plexiform neurofibroma
Fig. 4.165 |
MRI: T2 hyperintense with hypointense center (target sign). Heterogeneous CE. |
MRI best for tumor extent, especially when close to spine.
Assess for other manifestations of NF. |
Brachial plexus schwannoma |
MRI: Well-circumscribed, fusiform, T2 hyperintense enhancing mass between anterior and middle scalene muscles. T1 isointense.
CT: Isodense to muscle, calcification uncommon, moderate enhancement. Smooth, corticated widening of bony neural foramen. |
Painless, slow-growing mass in neck. May be indistinguishable from neurofibroma. |
Cervical thymus |
CT/MRI: At cervicothoracic junction, midline or to the left. Mimics appearance of normal thymus on all imaging modalities, and MRI may show connection with the mediastinal thymus. |
Incomplete thymic descent, usually asymptomatic but may cause dysphagia. |