The Pediatric Cervical Spine
Leonard E. Swischuk
John H. Harris Jr.
This chapter deals with trauma of the cervical spine in infants and children and how things differ from adults. It will not deal with all cervical spine fractures for many of them are no different than seen in adults. In addition, in the growing child especially the infant and young child, because of natural ligament laxity, hypermobility of the cervical spine abounds. As a result, many findings in infants and young children that would be considered abnormal in adults are normal.1, 2 Furthermore, the skeleton still is growing in children, and to accommodate this in the extra-axial skeleton, epiphyseal plates are present. In the spine, synchondroses serve the same function. If one is not familiar with these synchondroses, one may erroneously misdiagnose them for fractures. The most problematic of these occur in the second cervical vertebra and will be addressed later. This chapter also deals with congenital anomalies, which can go on to present in adulthood but often first present in the pediatric age group.
PREVERTEBRAL SOFT TISSUE SWELLING
Prevertebral soft tissue swelling often is difficult to evaluate because of problems in obtaining good images. To properly evaluate the soft tissues of the neck, the airway needs to be fully distended on inspiration and the neck needs to be extended. However, this can be difficult to accomplish, especially with the patient on the emergency medical service (EMS) backboard, but on the lateral view of the well-positioned normal airway, the posterior pharyngeal wall is always more posterior than the posterior tracheal wall and this results in a step-off of the air column at this level (Fig. 6.1A). This latter finding is helpful because even if the airway is not fully distended, if a step-off is retained, the findings likely are normal (Fig. 6.1B). When the study is obtained in expiration, tracheal buckling with a pseudomass frequently results (Fig. 6.1C) and the study needs repeating with proper technique (Fig. 6.1D).
In the end however, with all of this considered, I have come to this conclusion about the prevertebral soft tissues. If they are not sending a definite message, then do not spend too much time on them. Go on to evaluate the radiographs for signs of vertebral column instability. These include (1) anterior displacement of vertebral bodies (rotation-flexion injuries), (2) posterior displacement of vertebral body (hyperextension injury), (3) narrow disk space (flexion, rotational injuries), (4) wide disk space (hyperextension injuries), (5) pedicles seen “en face” (rotary subluxation), and (6) increased predental distance (C1-C2 dislocation).
SYNCHONDROSES
Synchondroses occurring in the third through the seventh cervical vertebra are not usually a problem. The problem is with synchondroses in the first and second cervical vertebrae.1, 2 With the first cervical vertebra, the problem is not as difficult for the synchondroses often are very symmetric, and once one appreciates this, there is little chance of misdiagnosing them for a fracture (Fig. 6.2).
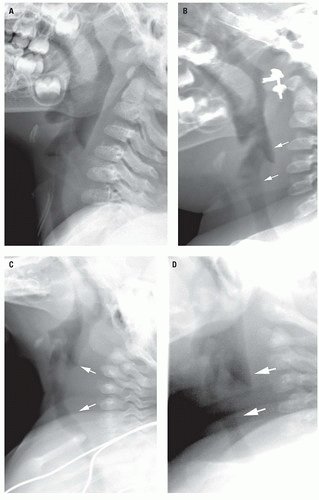 Figure 6.1. Airway: Normal and buckling. A: Normal fully distended airway in extension. Note that the posterior hypopharyngeal wall is posterior to the posterior tracheal wall. B: In this patient, thickening of the prevertebral soft tissues is suggested but because the step-off between the posterior pharyngeal wall and posterior tracheal wall is retained (arrows), the study likely is normal. This was a normal patient. C: Pseudomass (arrows) caused by the study being obtained during expiration. The neck is extended, but the study was obtained in expiration. D: With full inspiration, the airway is normal and the pharyngeal/tracheal step-off is retained (arrows). Even though the prevertebral soft tissues look a little prominent, the study is normal. |
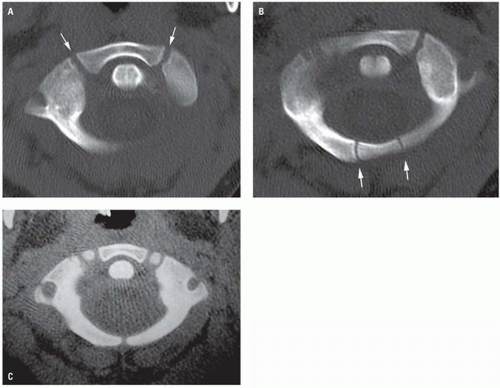 Figure 6.2. Synchondroses C1. A: Note symmetric anterior synchondroses (arrows). B: Similar posterior synchondroses (arrows). C: Numerous anterior and posterior synchondroses. |
The synchondroses of C2 are a different matter (Figs. 6.3A, 6.3B). Until one learns their configurations, it is very easy to misinterpret them for fractures. In previous days, on oblique views of the cervical spine, these synchondroses produced a Y-shaped radiolucent line configuration (Fig. 6.3C). With the advent of computed tomography (CT) imaging, the same configuration is seen on extreme lateral sagittal reconstructed views of the cervical spine (Fig. 6.3D). Aberrant synchondroses may appear very bizarre but they generally have smooth edges (Fig. 6.4).
NEURAL ARCH DEFECTS
Neural arch defects can be fractures or congenital defects. Fractures in the upper cervical spine usually result from hyperextension injuries such as the hangman’s fracture or axial loading injuries such as sustained in the Jefferson fracture of C1. The resultant defects usually are relatively thin and/or sharp-edged. They do not show sclerosis whereas congenital defects, although variable in their configuration, generally have smooth and sclerotic edges (Fig. 6.5).
Neural arch defects in the lower cervical spine are not particularly common.3, 4, 5 They are much more common at the C1 and C2 levels,1, 2, 6, 7, 8, 9, 10 but even here, they are much more common at the C1 level. At the C2 level, they need to be differentiated from hangman’s fractures, which do occur in infants and children.11, 12, 13, 14 In infants, these fractures maybe clinically silent and this is especially important because they can occur in the battered child syndrome.13, 14 C1 defects are very bizarre and extremely variable (Fig. 6.6). In spite of the bizarre and alarming appearance of all these defects, they are stable9, 15 and flexion/extension views can be confirmatory (Fig. 6.7).
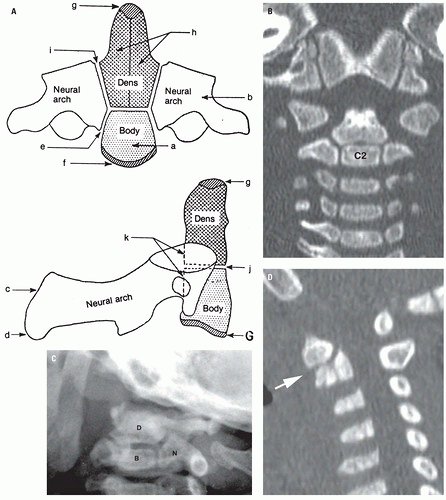 Figure 6.3. Synchondroses C2. A: Schematic representation of the ossification centers and synchondroses of the axis vertebra. The neurocentral synchondrosis is represented by e; the subdental (subchondral) synchondrosis, by j; and the synchondrosis between the dens and the neural arches, by i. (From Bailey DK. Normal cervical spine in infants and children. Radiology. 1952;59:713-714, with permission.) B: Coronal reconstruction of the C-spine demonstrates all of the synchondroses outlined in figure (A). Radiograph oblique view (C) demonstrates the triradiate synchondroses between the dens (D), body (B), and neural arch (N) of C2. Far lateral sagittal CT reconstruction (D) demonstrates the same findings (arrow). |
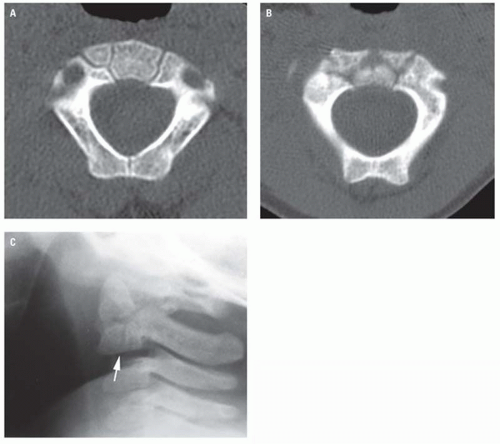 Figure 6.4. Aberrant synchondroses C2. A: Note the unusual, aberrant synchondroses of C2. B: In this patient, the aberrant synchondroses appear bizarre. C: Note the vertical synchondrosis (arrow) through the body of C2. |
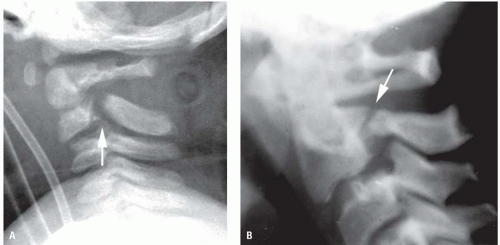 Figure 6.5. Posterior neural arch fracture verses defect. A: Hangman’s fracture in an infant (arrow). Note that the edges are sharp. B: Congenital defect (arrow) in a child. Note that the edges are smooth and slightly sclerotic. This spine was completely stable on flexion/extension. (continued) |
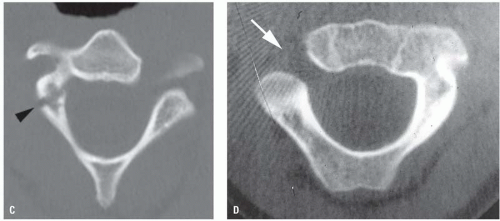 Figure 6.5. (continued) C: Hangman’s fracture on CT (arrow). Note that the fracture edges are very sharp and that there is no sclerosis. D: Congenital defect on CT (arrow) demonstrates smooth, sclerotic edges. |
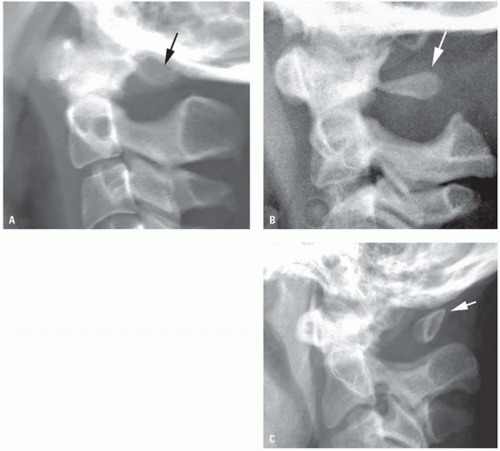 Figure 6.6. Underdeveloped/defective posterior arch of C1; variable appearance. A: In this patient, there is complete absence of the posterior arch of C1. B: This patient demonstrates a markedly underdeveloped posterior arch with only a smooth triangular shaped bony fragment remaining (arrow). C: This patient demonstrates only a residual spinous tip (arrow). All of these patients had stable spines. |
Having considered all of the foregoing, there is one exception to the rule of stability with posterior neural arch defects of the upper cervical spine. This exception occurs when the dens is congenitally hypoplastic.4 In such cases, the transverse ligaments that stabilizes the dens and the lateral masses of C1 are underdeveloped and weak. All of this leads to excessive motion at the C1-C2 level and an increase in the predental distance—all discussed in the next section. In such cases, even though one might first note that the posterior arch of C1 is hypoplastic or deformed when the hypoplastic dens is also noted, the whole problem takes on a completely different and more serious complexion (Fig. 6.8). It usually requires surgical stabilization.
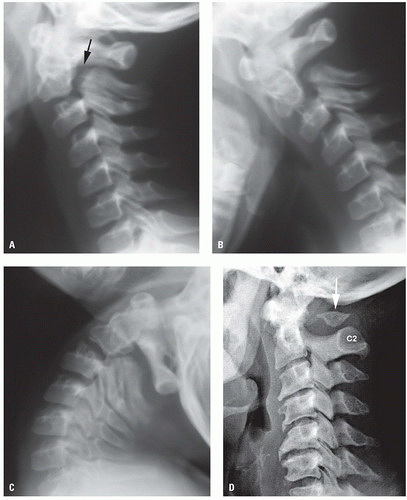 Figure 6.7. Congenital defect C1-C2; demonstration of stability. A: Note the smooth-edged defect (arrow) in the posterior arch of C2. C2 is slightly anterior-displaced and the disk space is wide anteriorly. B: With flexion, there is very little change in the width of the defect and C2-C3 alignments are basically unchanged. C: With extension, all of the vertebral bodies align up normally and there is very little evidence of excessive movement. This patient basically was stable but activity such as wrestling, football, gymnastics, and so forth might be discouraged. D: Note the underdeveloped posterior arch of C1 (arrow) and its relationship to the posterior arch of C2. This was a study in a 75-year-old male (note the degenerative changes in the mid-cervical spine region). (continued) |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


