Identify the compartments of the retroperitoneum and the fascia that divide them.
List the muscles, organs, and vessels normally found in each retroperitoneal compartment.
Differentiate between the location and function of the deep abdominal (parietal) nodes and the superficial (visceral) nodes.
List the indications for sonographic evaluation of the retroperitoneum.
Demonstrate the scanning techniques used to image the retroperitoneum.
Recognize the role retroperitoneal fascia play in identifying and limiting the extent of pathology.
Describe the six scanning objectives the sonographer should employ when retroperitoneal pathology is identified.
Differentiate the sonographic appearance of inflammatory and malignant adenopathy.
Describe the pathology, etiology, clinical signs and symptoms, and sonographic appearance of solid lesions and fluid collection found in the retroperitoneum.
Analyze sonographic images of the retroperitoneum for pathology.
Identify technically satisfactory and unsatisfactory sonographic examinations of the retroperitoneum.
KEY TERMS
abscess
adenopathy
AIDS
fibroma
fibrosarcoma
hematoma
HIV
leiomyoma
leiomyosarcoma
lipoma
liposarcoma
lymphocele
retroperitoneal fibrosis
rhabdomyoma
rhabdomyosarcoma
GLOSSARY
abscess a pocket of infection typically containing pus, blood, and degenerating tissue
adenopathy also called lymphadenopathy; enlargement of lymph nodes owing to inflammation, primary neoplasia, or metastasis
extravasate fluid, such as blood, bile, or urine, which is forced out or leaks out of its normal vessel into the surrounding tissues or potential spaces
fascia a thin sheet-like tissue that separates muscles
great vessels a term used to describe the aorta and inferior vena cava together
hematoma an extravasated collection of blood localized within a potential space or tissues
HIV human immunodeficiency virus; blood-borne virus that attacks T lymphocytes resulting in their destruction or impairment, eventually leading to AIDS
mass effect distortion or displacement of normal anatomy owing to a mass, neoplasm, or fluid collection
metastasis the spread of cancer from the site at which it first arose to a distant site
orthogonal planes that are perpendicular or at 90 degrees to each other
primary neoplasm a new growth of benign or malignant origin
urinoma an extravasated urine collection owing to a tear of the urinary collecting system
Sonography plays an important role in the examination of the retroperitoneum as well as the organs and vessels located within the cavity. Although computed tomography (CT) is the preferred imaging modality for retroperitoneal neoplasms and adenopathy, the radiation dose delivered to the patient over multiple examinations must be considered. Sonography produces high-quality images without ionizing radiation, it can provide real-time biopsy guidance, and it provides safe imaging for follow-up of disease progression or resolution. The skill and creativity of the sonographer often dictates the quality of the examination produced. A thorough knowledge of anatomy, pathophysiology, and sonography physics and instrumentation is required to produce the highest quality of sonographic examination. This chapter focuses specifically on the normal anatomy and pathologies found in the retroperitoneum.
ANATOMY OF THE RETROPERITONEUM
The parietal peritoneum is the outermost of two membranes that enclose most of the intra-abdominal contents, including the intestines, liver, pancreatic head, spleen, and pelvic organs. The other membrane, the visceral peritoneum, lies in direct apposition to the parietal membrane, thus forming a potential space. The area lying behind the peritoneal membrane is referred to as the retroperitoneum. The retroperitoneum is a complex abdominal space located between the parietal peritoneum and anterior to the transversalis fascia.1,2 It extends from the diaphragm superiorly to the pelvic brim inferiorly.3, 4 and 5
Retroperitoneal Compartments
The retroperitoneum is divided into three major compartments or spaces by the anterior and posterior perirenal fascia.6 These retroperitoneal compartments are the anterior pararenal space, the perirenal or perinephric space, and the posterior pararenal space.1,6,7 The fascial planes are fused superiorly but remain unfused caudally. The literature frequently refers to both the anterior and posterior as Gerota fascia, although it is more correct to reference the anterior renal fascia as Gerota fascia and the posterior renal fascia as Zuckerkandl fascia.8 The anterior renal fascia courses anterior to the great vessels, kidneys, and adrenal glands and extends across the midline to fuse with the posterior renal fascia laterally. The posterior renal fascia fuses with the anterior renal fascia laterally and tracks posterior to the kidney to blend with the anterior layer of the thoracolumbar fascia and the psoas fascial sheath medially.
An understanding of the retroperitoneal fascia is important to define the retroperitoneal compartments (Fig. 16-1A, B).
FIGURE 16-1 Retroperitoneum. A: A transverse sectional retroperitoneum illustration at the renal hilum level demonstrates the fascial planes and musculature relationship. B: The transverse drawing illustrates the three major compartments: anterior pararenal space (APR), perirenal space (PR), and posterior pararenal space (PPR). K, kidney; P, pancreas; RF, renal fascia.
Anterior Pararenal Space
The anterior pararenal space is bordered anteriorly by the posterior parietal peritoneum and posteriorly by the anterior perirenal fascia.6 The space communicates with the opposite side around the pancreas.1 Inferiorly, this space communicates with the extraperitoneal space of the pelvis and the posterior pararenal space.9 The communication is important because it allows cells and fluid to travel between the two spaces. Along with a variable amount of fat, some portions of the digestive organs are embedded in this layer including the pancreas; distal common bile duct; the second, third, and fourth parts of the duodenum; and the ascending and descending colon.10
Perirenal or Perinephric Space
The perirenal space is bordered anteriorly by the anterior renal fascia and posteriorly by the posterior renal fascia. Superiorly, the fascias fuse and attach to the diaphragmatic crura bilaterally immediately superior to the adrenal glands. Inferiorly, the perirenal space is open at the level of the pelvic brim because the fascial perirenal sheaths remain unfused. The perirenal space encloses the kidneys, adrenal glands, perinephric fat, and the prevertebral aorta and inferior vena cava (IVC).1,10
Posterior Pararenal Space
The posterior pararenal space lies between the posterior renal fascia and the transversalis fascia. This space contains no organs, only fat.10 The retrofascial space is located immediately posterior to the posterior pararenal space and it contains the psoas muscle posteromedially and the quadratus lumborum muscle posteriorly. The retrofascial space is not technically part of the retroperitoneum, but its muscles are frequently referred to in discussions of the retroperitoneal space.
Table 16-1 lists the organs and vessels contained in the retroperitoneum.
ANATOMY OF THE LYMPHATIC SYSTEM
The lymphatic system extends throughout the body with lymph vessels found immediately adjacent to normal arteries and veins.7,11 Unlike the vascular system, the lymph vessels end in a blind-ending plexus of tubes at the vascular capillary level. The lymphatic system acts as a fluid recovery system, collecting nearly 3 L of plasma fluid that oozes from the normal vascular capillaries into the extracellular space. The lymphatic system also collects cellular debris and bacteria within the extracellular fluid, as well as absorbing and transporting dietary fat. Because the lymphatic system returns excess fluid to the bloodstream, homeostasis (internal fluid balance) is maintained.
TABLE 16-1 Retroperitoneal Organs and Structures
Diaphragmatic Crura
Aorta
Pancreas
Inferior vena cava
Distal common bile duct
Superior mesenteric artery
Second, third, and fourth parts of duodenum
Superior mesenteric vein
Kidneys
Hepatic artery
Adrenals
Splenic artery
Lymphatic vessels and nodes
Splenic vein
The fluid that enters the lymphatic plexus is referred to as lymph. This thin, colorless, or slightly yellow fluid has a cellular composition similar to blood plasma. Lymph flows from the lymph capillary plexus toward the great vessels in the abdomen, eventually to the right and left subclavian veins in the thorax. The right lymphatic duct conducts lymph collected from the right head, neck, arm, and chest back into the venous system at the confluence of the right internal jugular and the right subclavian vein. The thoracic duct conducts lymph collected from the rest of the body back into the venous system at the confluence of the left internal jugular and the left subclavian vein. The chyle cistern is a dilated collecting area found in the midretroperitoneum that collects lymph from the lower extremities and pelvis before it ascends to the thoracic duct7,11 (Fig. 16-2A, B).
Lymph moves through lymphatic vessels, passing through lymph nodes along the way. Each lymph node is a small mass of lymphatic tissue that filters the lymph fluid, phagocytizing foreign proteins and infectious debris, and generating and sending lymphocytes to infected tissues. Lymph nodes are described based on their location. See Table 16-2 for a list of commonly affected abdominopelvic lymph node groups and measurements that indicate abnormal size.
In the retroperitoneum, lymph nodes are generally divided into deep abdominal or parietal lymph nodes and superficial abdominal or visceral lymph nodes. Parietal nodes are those lymph nodes found in the retroperitoneum surrounding the principal blood vessels. They are grouped according to the arterial vessel with which they are associated. In the upper retroperitoneum, aggregations can be found around three unpaired vascular branches: inferior mesenteric, superior mesenteric, and celiac. Groups found in the lower retroperitoneum include the external, common, internal iliac, and epigastric.
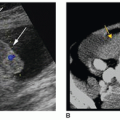
Nodes are positioned 360 degrees around the aorta and IVC. Those that lie posterior to the great vessels (aorta and IVC) provide the most reliable indicator of lymphadenopathy because they frequently displace the aorta or IVC anteriorly (Fig. 16-3).
Visceral nodes are located within the peritoneal cavity and are generally found at the hilum of organs. The most common groups are gastric, hepatic, pancreatic, splenic, and various groups associated with branches of the colic artery.
A special type of lymph node found along the small bowel and mesentery are called lacteals. Lacteals take on a milky white appearance because they also absorb dietary fat.
SCANNING TECHNIQUE AND NORMAL SONOGRAPHIC APPEARANCE
Ideally, patients should be fasting for 6 to 8 hours prior to the examination. This will reduce bowel gas and fluid that may be confused with pathology; however, if needed, an examination of the retroperitoneum may be performed without any patient preparation. Owing to the retroperitoneum’s deep position, a 3-to-6-MHz sector or curvilinear transducer should offer adequate penetration and a wide field of view for most adult retroperitoneal examinations. Higher-frequency transducers should be used on smaller children whereas lower-frequency transducers provide better penetration on obese patients.
FIGURE 16-2 Lymphatic system. This illustration shows the parietal node groups of the abdominopelvic cavity and their relationship to the blood vessels. (Reprinted from Moore K, Dalley A, Agur A. Clinically Oriented Anatomy. 6th ed. Lippincott Williams & Wilkins; 2010:316, with permission.)
Encircling the aorta (periaortic) or inferior vena cava (pericaval) or both (interaortocaval)
>10
Mesenteric and celiac
Anterior to the abdominal aorta surrounding the origins of the celiac axis and mesenteric arteries
>10
Pelvic
Along the common, external and internal iliac (hypogastric) arteries and veins; also referred to as the iliac chain
>15
Intraperitoneal
Gastrohepatic
Within the superior portion of the lesser omentum that suspends the stomach from the liver
>8
Perisplenic
At the splenic hilum
>10
Parapancreatic
Between the duodenal sweep and the pancreatic head anterior to the inferior vena cava
>10
Hepatic hilum
Surrounding the porta hepatis
>6
The retroperitoneum may be scanned using an anterior, coronal, or posterior approach. The anterior approach frequently involves directing the sound beam through the left lobe of the liver in the epigastric region or through a fluid-filled stomach when overlying bowel gas obstructs visualization of deeper anatomy. Coronal scan planes are frequently used, directing the beam through the liver on the right and the spleen on the left, to evaluate kidneys, adrenals, and midline retroperitoneal structures that are not seen well from an anterior approach. The posterior or flank scanning approach may be employed, directing the ultrasound beam through the deep back muscles (see Fig. 16-1), when the anterior and coronal approach offer less than desirable imaging. Rolling the patient into oblique, decubitus, and prone positions using the above scanning approaches will shift air and organ position and potentially improve imaging.
Only gold members can continue reading. Log In or Register to continue