8
The Value of PET/CT
Eugene C. Lin, Paul E. Kinahan, and Abass Alavi
Positron emission tomography combined with computed tomography (PET/CT) has tremendous potential, as it combines the most sensitive imaging modality (PET) with the highest resolution cross-sectional imaging modality (CT). The addition of fused CT to PET images has numerous advantages over PET alone, but the interpreter should be aware of potential pitfalls introduced by the process of CT fusion and attenuation correction in PET.
- Increased accuracy. PET/CT adds a substantial incremental benefit compared with using PET alone, and to a lesser extent compared with side-by-side reading of PET and CT. In one study,1 only 52% of pathologic lesions were accurately characterized (localization and infiltration of adjacent structures) by PET alone. The remaining 48% required either side-by-side CT reading or combined PET/CT. However, many of the cases that may require CT correlation can be accurately interpreted with side-by-side reading of PET and CT. In ~6 to 12%1,2 of total PET cases, side-by-side reading is not adequate for either accurate lesion localization or characterization, and combined PET/CT may be needed for these purposes. In tumor staging, PET/CT has an incremental 8% increase in accuracy relative to PET and side-by-side CT interpretation and a 20% increase relative to PET interpretation alone.3
- Specific advantages. PET/CT provides the same advantages that can be achieved by correlating any type of functional and structural imaging techniques (see Chapter 7). PET/CT maximizes these advantages by providing the most accurate correlation. The improved accuracy achieved is noted in
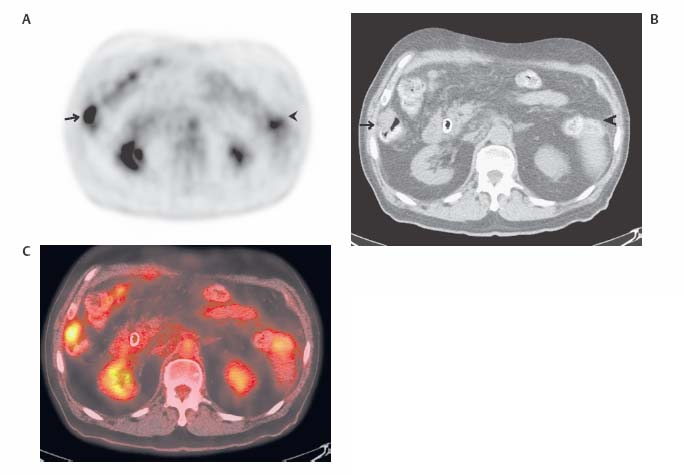
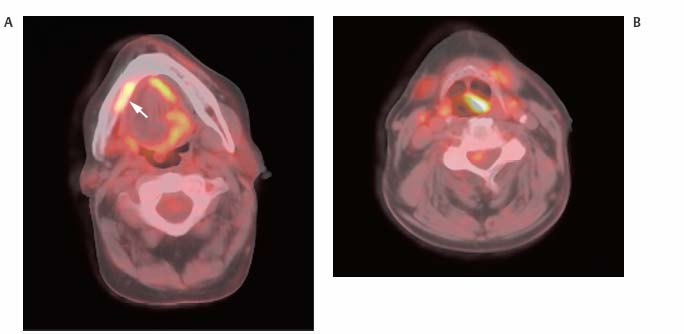
- Localizing lesions (Fig. 8.1)
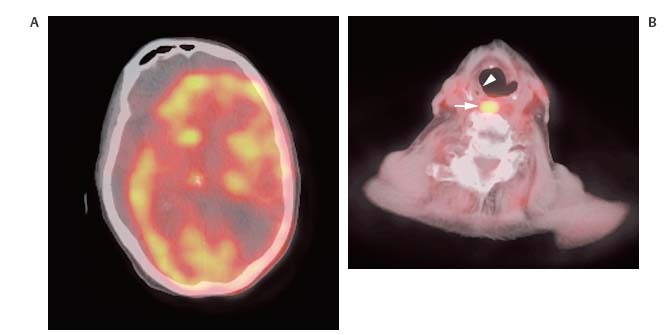
- Identifying false-positive findings (Fig. 8.2)
- Determining the nature of subtle or equivocal PET findings and therefore improving the degree of certainty of the results (Fig. 8.3)
PET/CT usually enhances the specificity rather than sensitivity compared with PET alone. Many sources of false-positive findings are easily identified by PET/CT. However, sensitivity can also improve with PET/CT. For example, areas that may be thought to definitely or questionably represent physiologic activity on PET alone can be shown to localize to a pathologic sites on the fused CT scan. The color images used to interpret PET/CT can also make some lesions more conspicuous.
- Contemporaneous correlation. Although side-by-side CT correlation is often adequate, the CT studies are often not contemporaneous. This can result in errors (as seen in Fig. 7.7, p. 85) from changes that have taken place during the time interval between acquiring the CT and the PET scan. This issue is obviated with PET/CT.
- CT-based attenuation correction for PET. The CT scan can be used for attenuation correction of PET data4, allowing for decreased scan time, as the CT is completed more quickly than a radionuclide source scan. In addition, PET image noise is reduced due to the decreased noise of the CT relative to a radionuclide source scan and the lack of postemission contamination on transmission images.
- PET/CT artifacts. The only disadvantages of combined PET/CT relative to PET alone are the artifacts specific to PET/CT (see Chapter 30 for a discussion of artifacts specific to cardiac PET/CT). These artifacts are primarily related to three factors:5
- Misregistration due to differences in position of structures between PET and CT
- Artifacts due to differences in attenuation of structures between PET and CT
- Truncation artifacts related to the CT field of view diameter (typically 50 cm) differing from the larger PET field of view diameter (typically 70 cm). All manufacturers are addressing this issue by allowing for reconstruction of an extended CT field of view.
Misregistration artifacts are most prominent in areas of greatest respiratory motion—the lung bases and the diaphragmatic region. Misregistration results in two basic artifacts:
- Incorrect uptake levels. Motion between PET and CT results in inaccurate attenuation correction, as the region on CT used for attenuation correction does not correspond exactly to the region on PET. This can result in artifactually decreased or increased visual levels of uptake and inaccurate calculation of standardized uptake value (SUV).
- Mislocalization. Lesions can be localized to the wrong location on fused PET/CT images.
- Type of respiration. In a combined PET/CT study, the CT scan can be acquired during free (shallow) breathing, maximum inspiration, and normal expiration. The PET scan must be acquired during free breathing due to the length of the scan. The type of breathing during the CT will affect the incidence of artifacts.6 Mislocalizations from respiration will usually be in the superior to inferior dimension.
- Normal expiration. This will usually result in the most accurate fusion, as most of the breathing cycle is spent in expiration. This may be the preferred protocol with fast CT scanners. Scanning in normal expiration is preferred, but may not be possible, as some patients may not be able to breath-hold in normal expiration for the duration of the CT.
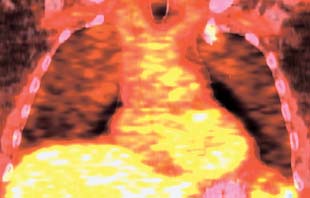
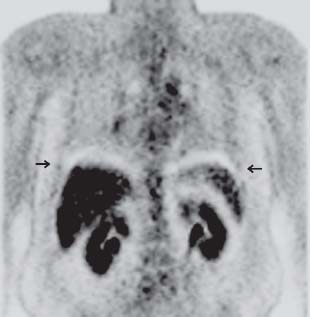
- Inspiration. Inspiratory maneuvers, whether a small or regular breath in, will typically result in the most significant misalignment of PET and CT at the diaphragm and heart.7 Inspiration can cause photopenic curvilinear artifacts at the lung–diaphragm interface (Fig. 8.4). This occurs because measured attenuation in this region is too low (there is only lung in this region on the maximum inspiration CT, whereas subdiaphragmatic structures are present in the same region on PET), leading to undercorrection of the detected activity in this region. Photopenic artifact can also be seen at the interface between the heart and the lungs (Fig. 8.5).
- Free breathing. Free breathing can also cause photopenic curvilinear artifacts at the lung–diaphragm interface if the peridiaphragmatic area is scanned during inspiration. However, image coregistration with shallow breathing is typically superior to that with inspiration.7
- Corrections for respiratory misregistration
- Respiratory averaged low-dose CT scanning. For some PET/CT scanners, this method uses cine-CT acquisition to form a respiratory-blurred CT-based attenuation correction image. This potentially reduces the mismatch with the respiratory-blurred PET image.8 The low-dose respiratory-blurred CT image is not viewed, and care must be taken to use as low CT technique factors as possible to avoid excessive radiation dose to the patient.
- Respiratory gating. Four-dimensional PET/CT protocols with respiratory gating can improve the spatial matching between PET and CT, but they often require long acquisition and postprocessing times. Other protocols9 have been developed that might improve registration with minimal acquisition and postprocessing time and effort.
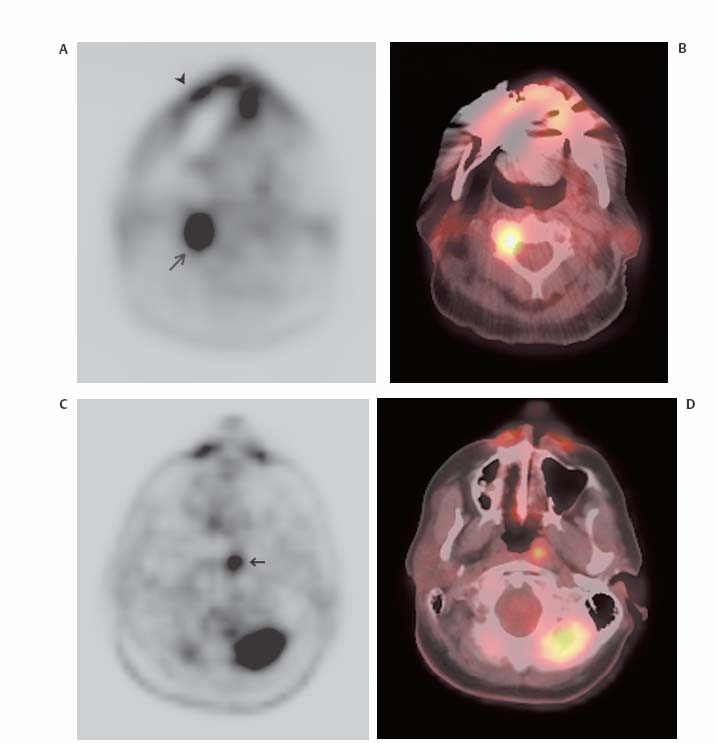
- Nonrespiratory motion. This is most commonly seen in the head and neck where motion between the CT and PET scans results in mislocalization mostly in the medial to lateral dimension (Figs. 8.6 and 8.7). Another area where this is commonly seen is the breast (Fig. 8.8). On some systems this can be corrected (on the scanner console) by realignment tools.
- SUV. Areas of artifactually decreased and increased activity and therefore inaccurate SUV measurements have been described in the lung bases and bowel. This can result in both a false-positive and a negative interpretation of the resulting images.
- Lung bases. The SUV can be altered by up to 30%.
- Bowel. Differences in bowel motion between PET and CT from peristalsis and respiration can result in areas of falsely increased or decreased activity and SUVs on CT attenuation-corrected imaging. This could result in reduced sensitivity for detecting adjacent malignant peritoneal implants and nodes, or false-positive findings (Fig. 8.9). Areas of artifactually reduced activity are more common than those with increased activity.10
 Advantages
Advantages Disadvantages
Disadvantages