2University of Athens, Athens, Greece
3The London Independent Hospital, London, UK
- The TS and LS are better protected than the CS
- Larger forces are necessary to cause serious injuries
- Spinal injuries are often associated with injuries elsewhere
- In major trauma, TS and LS CT is covered as part of the whole body CT protocol
- MRI is indicated if there is suspicion of neurological, ligamentous or disc injury
Injuries to the thoracic and lumbar spine (TS and LS) commonly occur as a result of high-energy trauma such as falls from a height or motor vehicle collisions with axial loading, hyperflexion, extension, distraction, rotation or shearing forces. Lower energy trauma such as simple falls can result in significant injury, particularly where there is a predisposing condition such as osteoporosis, ankylosing spondylitis or spinal metastases. Patients may present with specific signs or symptoms suggesting injury to the spine such as back pain or a cauda equina syndrome. Most significant injuries are encountered in victims of major trauma who may have other life-threatening injuries. Clinical examination of the thoracic and lumbar spine is part of the secondary survey and is deferred until life-threatening conditions have been stabilised. Clinical evaluation can be misleading, especially in patients with other distracting injuries and is of limited value in unconscious patients. In these patients, CT of the TS and LS is covered as part of the whole body CT protocol.
Spinal injuries may be either stable or unstable with risk of mechanical or neurological deterioration. Injuries should be assumed to be unstable with appropriate immobilization and log rolling, until fully assessed by an experienced clinician and appropriate imaging has been performed.
Anatomy (Figure 11.1)
There are normally 12 thoracic (Figure 11.2) and 5 lumbar vertebrae (Figure 11.3); however, variations are relatively common and it can be difficult on imaging to determine which are the T12/L1 or L5/S1 vertebrae. This is due partly to variation of the 12th ribs, but mainly to the presence of transitional vertebrae (Figure 11.4) at the lumbosacral junction with partial sacralisation of L5 or partial lumbarisation of S1. Six lumbar vertebrae may also occasionally be present. If images of the TS and LS are available then levels can be determined by counting down from T1; however, this may be further complicated by the presence of cervical ribs. The longest and most horizontal transverse processes are usually at L3.
Figure 11.1 Anatomy of lumbar spine: lateral LS and drawing. 1, ALL; 2, IVDS; 3, interspinous ligament; 4, PLL; 5, inferior articular facet of L4; 6, superior articular facet of L3; 7, pedicle of L4; 8, pars interarticularis of L4; 9, ligamentum flavum; 10, spinous process of L3.
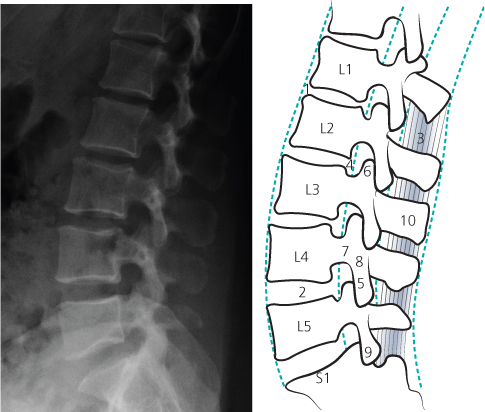
Figure 11.2 (a) Normal AP and (b) lateral views of the thoracic spine.
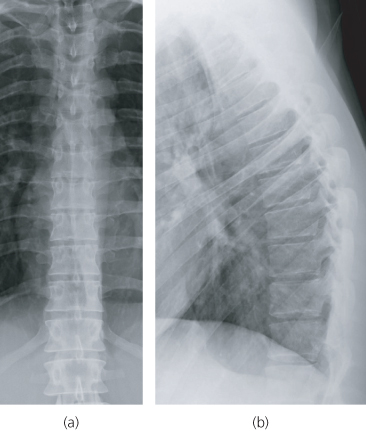
Figure 11.3 (a) Normal AP and (b) lateral views of the lumbar spine.
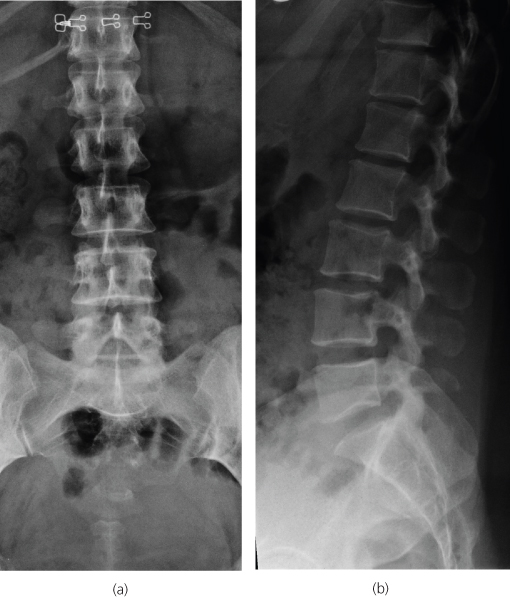
Figure 11.4 AP view of the lumbar spine demonstrating a transitional lumbosacral vertebra with articulation on the left side (Bertolotti’s syndrome if patient is symptomatic).
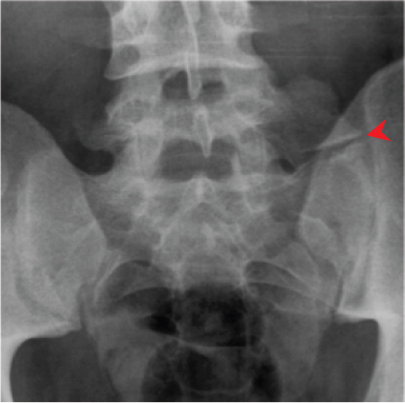
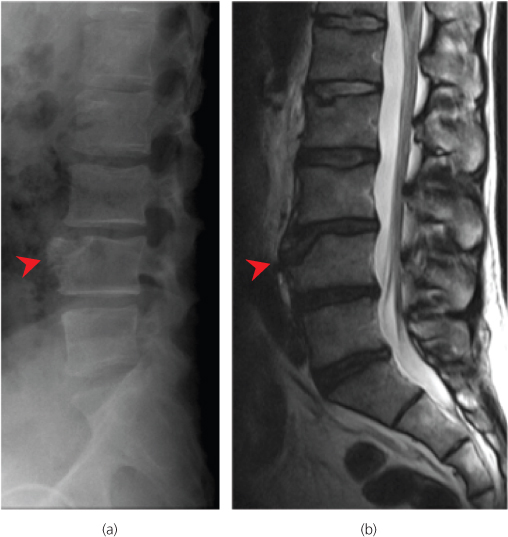
Figure 11.5 (a) Lateral radiograph and (b) sagittal T2 weighted MR image demonstrating an L4 limbus vertebra.
Each vertebrae comprises a body and spinous process, plus two paired pedicles, transverse processes, superior and inferior articular facets, pars interarticularis and laminae. In the TS, there are articular facets on the lateral aspect of the vertebral bodies for articulation with the ribs. The lumbar vertebral bodies are larger and have a more horizontal spinous process.
Numerous strong ligaments support the spine, including the anterior and posterior longitudinal ligaments, the ligamentum flavum, and the interspinous and the supraspinous ligaments. The thoracic column is also stabilised by the upper ribs which form the thoracic cage. The lower ribs and the LS have strong surrounding muscles which augment the intrinsic stability provided by the discs, ligaments and facet joints.
The transition between the relatively immobile TS and the more flexible LS renders the thoracolumbar junction relatively vulnerable to injury, and around 60% of all injuries occur between T11 and L2. Upper and mid TS injuries are relatively uncommon in adults. By contrast, children have a relatively more mobile spine and injuries are most common at T4/5 and L2. The injuries are often multiple and contiguous.
Congenital vertebral anomalies such as hemivertebrae and butterfly vertebrae, or limbus vertebrae (Figure 11.5) due to non-fusion of the ring apophyses, can be confusing and may be mistaken for acute fractures.
The spinal cord terminates at the conus medullaris, which usually lies between T11 and L2. Below this level, neurological injuries are lower motor neurone due to nerve root injury, whereas more proximal spinal cord injuries are upper motor neurone resulting in hyperreflexia, spinal shock and spasticity.
Mechanism of injury
There are several definable force vectors, which can result in spinal trauma, producing predictable patterns of injury (Box 11.1). Injuries are frequently the result of hyperflexion with forced bending around a fulcrum centered on the posterior third of the vertebral body. This produces anterior vertebral compression fractures (Figure 11.6) and when severe is associated with posterior element distraction (Figure 11.7). Axial loading for example due to a fall from a height produces compressive forces which result in burst fractures of the vertebral body (Figure 11.8). Hyperextension, rotation and shearing forces also produce defined patterns of injury although in many cases injuries are due to a combination of forces such as hyperflexion and axial loading, or flexion and rotation.
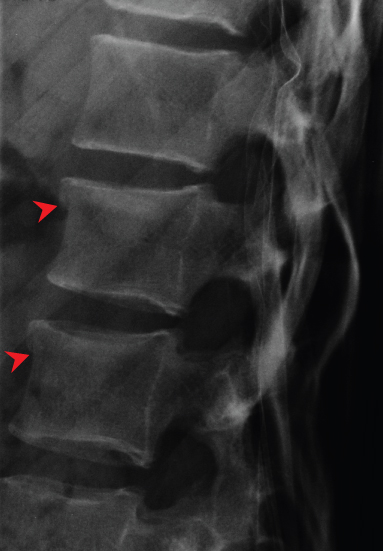
Figure 11.6 Lateral radiograph demonstrating minor anterior wedge compression fractures of L1 and L2.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


