Chapter 25 Thoracic Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Thoracic medial branch nerve radiofrequency neurolysis is indicated for the treatment of axial thoracic (i.e., mid back) pain that typically originates from zygapophysial (i.e., facet) joint sprains, contusions, or osteoarthritis. This procedure is performed via a posterior approach. The tip of the radiofrequency needle is placed at the superior lateral edge of the transverse process in an oblique fashion so that the tip bisects the superior lateral edge. The labeling and location of the thoracic medial branch nerves are covered in Chapter 24. Thoracic zygapophysial joint pain must first be confirmed through controlled diagnostic medial branch nerve blocks (see Chapter 24) before considering radiofrequency neurolysis for the treatment of such pain. Two medical branch nerves must be denervated to render a thoracic zygapophysial joint painless. For example, the T5 and T6 medial branch nerves must be denervated to treat pain that originates from the T6-T7 zygapophysial joint.
This chapter will focus on the radiofrequency technique for neurolysis of the thoracic medial branch nerve. As discussed in Chapter 24, the location of the medial branch nerves in relationship to the transverse process varies anatomically, depending on the thoracic level. The variability of the location of the medial branch nerves is greatest in the mid thoracic spine region (i.e., T4-T8) (Figure 24–5).1 An injection of a phenol solution has been used to create a chemical neurolysis of the median branch nerves.2 Although there is a lack of medical evidence in the literature, the injection of phenol has been used either alone or in combination with radiofrequency to denervate cervical, thoracic, and lumbar medial branch nerves.
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
 Trajectory View (Figure 25–1)
Trajectory View (Figure 25–1)
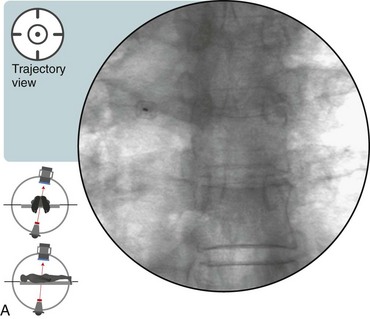
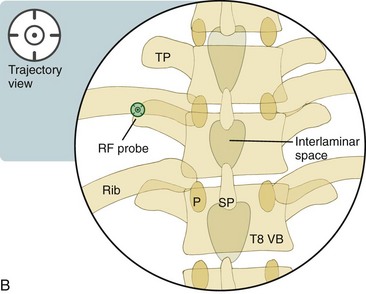
 Notes on Positioning in the Trajectory View
Notes on Positioning in the Trajectory View


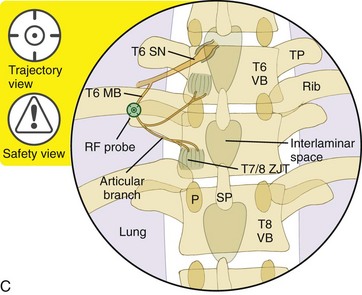
 Anteroposterior View Safety Considerations
Anteroposterior View Safety Considerations
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
 Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


