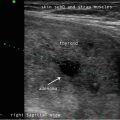
Fig. 32.1
Laryngeal anatomy on ultrasonography
It is important to clarify the orientation of the VC visualization on US versus FL which can be confusing because the right VC is displayed on the right of the screen on both studies, although the arytenoids are on the opposite sides of the screen. On VCUS , the arytenoids are on the inferior portion of the screen, and on FL it is on the superior portion of the screen. This orientation of VC visualization between both studies is further explained on Video 32.3.
32.3 Technique and Material
The patient’s position for VCUS is similar to the cervical hyperextension used for scanning of the thyroid gland (Fig. 32.2). The probe is placed just inferior to the thyroid cartilage angling superiorly (Fig. 32.3). Ample gel should be used to obtain ideal probe contact with the trachea and thyroid cartilage.


Fig. 32.2
Patient’s position for vocal cord ultrasonography
Fig. 32.3
Probe position on the patient’s neck for VCUS
Ultrasound probe for small parts scanning with capability to decrease its frequency from 15 to 12 MHz to 8–9 MHz is necessary to improve the visualization of TVC. Higher frequencies will decrease the ability to visualize the arytenoids and the hyperechoic TVC , especially posteriorly. Furthermore, the gain should be increased to enhance the visualization of the structures posterior to the thyroid cartilage.
TVCs can be visualized during passive breathing and phonation; however, localization and rapid evaluation of bilateral VC movement can be accomplished by asking the patient to perform a Valsalva maneuver. During Valsalva, the TVC will adduct on the midline allowing the ultrasonographer to easily localize the VC by slightly moving the probe superiorly and inferiorly. When the TVCs are found closed on the midline, the patient is asked to take a normal breath and TVC , FVC and arytenoids will abduct, therefore confirming bilateral vocal cord mobility as seen on Videos 32.4 and 32.5.
Usually when a TVC is paralyzed, ipsilateral FVC and arytenoid cartilage are also immobile as seen on Video 32.6 where the right TVC is paralyzed. A valuable hint of vocal cord dysfunction is the asymmetry of the arytenoids as seen on this clip. Video 32.7 shows left immobile TVC demonstrating similar findings. On both videos, arytenoid cartilage asymmetry and immobility of TVC , FVC , and arytenoid are easily visualized.
Frequently, not all structures can be visualized at the same time which might be one of the reasons for the variation TVC visualization rates among ultrasonographers. It is more challenging to demonstrate the TVC than the FVC and arytenoids. While the arytenoids are anatomically accurate predictors of TVC function, Wong et al. have shown that FVC movement on US also predicted the TVC mobility [13]. Further studies are needed to validate this finding since FVC can be hyperfunctioning when there is a TVC paralysis. In the author’s opinion, arytenoid cartilages asymmetry is an accurate marker of abnormal vocal fold movement and it should raise the suspicion for VC mobility dysfunction; however, immobility of TVC and/or arytenoids should be used as diagnostic of VC paralysis.
32.4 Pearls and Pitfalls of Vocal Cord Ultrasound
VCUS has significant limitations which are mainly associated with inability of vocal folds visualization in patients with thyroid cartilage calcification (TCC) (Fig. 32.4). Because most men have thyroid cartilage ossification, VCUS has a very low visualization rate in men.

Fig. 32.4
 Ultrasound-Guided Laser Ablation
Ultrasound-Guided Laser Ablation
 Transcutaneous Laryngeal Ultrasonography: Clinical Variables
Transcutaneous Laryngeal Ultrasonography: Clinical Variables
 Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
 Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
 Feature Illustration: Vascularity
Feature Illustration: Vascularity
 Pattern Recognition: Diffuse Thyroid Disease
Pattern Recognition: Diffuse Thyroid Disease




Demonstrate thyroid cartilage calcification
Related posts:
Ultrasound-Guided Laser Ablation
Transcutaneous Laryngeal Ultrasonography: Clinical Variables
Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
Feature Illustration: Vascularity
Pattern Recognition: Diffuse Thyroid Disease
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
