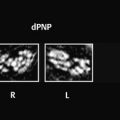
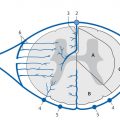
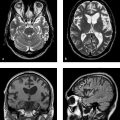
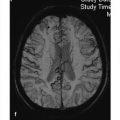
The indication for MRI in acutely spine-injured patients is decided on an interdisciplinary basis. Positioning and monitoring are highly demanding and require special care and attention. The anesthesia unit and monitoring techniques must be MRI-compatible. Modern MRI systems can significantly shorten the examination times. Faster sequences will reduce motion artifacts. Despite recent innovations, spin echo (SE) sequences are still the standard, although acquisition times have been shortened by the use of turbo spin echo (TSE) technique with T1w and T2w sequences. It is known that T1w sequences bring out anatomic details while T2w sequences are better for detecting normal and abnormal fluid collections in the form of hemorrhage or edema. The STIR sequence is very sensitive to edema and should always be included in the protocol for spinal trauma. With its fat suppression and accentuation of fluids, STIR imaging is also useful for detecting microfractures with associated bone marrow edema. All investigations for bleeding within the spinal cord require gradient echo (GRE) sequences. T2*w sequences, with their high sensitivity to susceptibility artifacts, are of key importance in the detection of blood breakdown products. This is of interest not only in acute injuries but also in disability evaluations. GRE sequences should not be used in patients with fractures already stabilized with internal fixation materials, because artifacts would hamper image interpretation. The following sequences should be routinely included in the MRI protocol for spinal injuries: T1w and T2w images in sagittal planes using TSE sequences. Axial GRE or T2*w images at the level of interest, particularly in the cervical spine (T2w TSE images are preferred for the thoracic spine). STIR sequences in the sagittal plane (less commonly the coronal plane) for the sensitive detection of fractures and edema. The following images may also be appropriate, depending on individual findings: T1w and PDw or T2w coronal images at the craniocervical junction for evaluating the dens; images may also be angled along the alar ligaments if desired. MR myelography for the evaluation of suspected root sleeve injuries. Magnetic resonance angiography (MRA) for the evaluation of suspected injuries to cerebral supply arteries caused by trauma to the cervical spine. Intravenous contrast administration is rarely indicated in the acute phase after spinal trauma. It should be used only if problems arise in differentiating hematomas from inflammatory or neoplastic changes in patients with an unclear history. Contrast administration is more often used for the detection of possible inflammatory complications in the late phase and during postoperative follow-ups. The diagnosis of acute injuries to the spinal column including the intervertebral disks, ligament attachments, and facet joints presents a challenge for the radiologist. The detection of spinal instability is essential for further treatment planning, as it will generally require surgical intervention. If neurologic symptoms are already present, their cause must be ascertained. Conventional radiographs cannot detect all relevant injuries with high confidence under emergency conditions. In particular, regions like the craniocervical junction and cervicothoracic junction continue to be a problem. Due to the nature of the modality, ligament instabilities cannot be definitively assessed in standard views. Thus, approximately one-half of all discoligamentous instabilities in the cervical spine are missed on conventional radiographs. As a result, CT has become established in recent years as the modality of choice for imaging the spinal column. The need for CT in any given case will depend on the trauma mechanism, clinical presentation, and conventional radiographic findings. The current S3 guideline on multiple injuries issued by the Association of Scientific Medical Professional Societies (AWMF) lists the following criteria indicating a high probability that multiple injuries have been sustained: Fall from a height of more than 3 m. Driver or passenger thrown from a motor vehicle. Passenger death. Pedestrian or bicyclist struck by a motor vehicle. Automobile or motorcycle crash at relatively high speed. Entrapment or crush injury. Explosion injury. High-energy collision (with vehicle deformation). Polytrauma CT has become the mainstay for imaging cases of this kind. Ideally the patient is examined with a multislice CT scanner (16 or more detector rows), which can provide full coverage of the spinal column with acceptable resolution and allows for secondary reconstructions. It is important to scrutinize the CT images for potentially subtle signs of a serious injury to the spinal column, which in turn would be an indication for MRI. Thus, MRI has only selected indications in acute posttraumatic examinations: Neurologic findings of unknown cause that are not explained by available CT scans (i.e., a discrepancy exists between clinical manifestations and imaging findings). Positional abnormalities in the spinal column, especially with involvement of facet joints ( ▶ Fig. 13.1). Presumed ligament lesions such as bony avulsions (teardrop fractures) that suggest additional ligamentous injuries. Fracture patterns in vertebral bodies that suggest a high likelihood of associated soft-tissue injury, such as flexion and extension injuries that are probably associated with posterior tissue disruption in addition to anterior longitudinal ligament injury. Selected cases where surgeons desire preoperative visualization of the spinal cord and epidural fluid collections. Visualization of the spinal cord before stabilizing procedures in patients who cannot be examined neurologically; also for medicolegal reasons, in order to differentiate preoperative from postoperative changes. Evaluating nerve root damage in patients with traumatic radiculopathy. Reducing radiation exposure in children with an unexplained trauma mechanism. Whether MRI is used acutely or postacutely depends on the patient’s overall status. The treatment of life-threatening intracranial or intra-abdominal injuries in multiply injured patients would take precedence over immediate MRI. Fig. 13.1 CT and MRI following high-impact trauma. The patient required primary intubation. His neurologic status was unclear. (a) Midsagittal reformatted CT image shows slight posterior gaping of the C5–C6 disk space. (b) Suspicion of injury to this segment is supported by incipient subluxation of the facet joint. (c) MRI demonstrates a complete rupture of all ligaments and the intervertebral disk with severe instability. Note MRI should never replace CT for the evaluation of spinal injuries in adults. CT is best for the classification of acute bony injuries, which tend to be overinterpreted on MRI. Segments adjacent to an acutely fractured vertebral body show extensive cancellous bone edema, which may be present at multiple levels ( ▶ Fig. 13.2). Fig. 13.2 Acute compression fracture of the T8 vertebral body after a fall from a bicycle. Sagittal STIR image of the thoracic and lumbar spine: repetition time (TR) = 2500, echo time (TE) = 70, inversion time (TI) = 170. Radiographs of the spine revealed a compression fracture of the T8 vertebra (arrow). The edema-sensitive STIR sequence additionally shows pathologic changes in almost all the thoracic vertebral bodies in proximity to endplate microfractures. Because CT and MRI are static imaging studies, selected cases will additionally require dynamic evaluation by fluoroscopy. An experienced clinician will conduct the examination under direct roentgen control to detect dynamic instabilities. Functional views should not be obtained “blindly” under any circumstances. Dynamic MRI studies also have no role in acutely spine-injured patients and are contraindicated during the acute phase. Isolated atlanto-occipital dislocation, which is not necessarily associated with a fracture, leads to a high, complete cord lesion or immediate death. Atlanto-occipital subluxation is also a serious injury. Often it is associated with a fracture, particularly of the atlas, and this may be combined with tears of the transverse ligament. Important stabilizing elements in this region are the joint capsule, the tectorial membrane, which extends from the posterior longitudinal ligament to the inner surface of the occiput, and the transverse ligament, which binds the dens to the anterior arch of the atlas. MRI can demonstrate several of these ligaments and the effects of their injuries ( ▶ Fig. 13.3a, b). In interpreting sagittal MR images, it is important not only to evaluate median and paramedian structures but also analyze the relationship of the occipital condyles to the atlas in more lateral planes. It is essential, therefore, to prescribe a suitable slice package that will cover this region. The relationship of the dens to the skull base is best evaluated in the coronal plane. Fig. 13.3 Atlantoaxial dislocation after a motor vehicle accident. (a) Sagittal T2w TSE image of the head and craniocervical junction. A complete discontinuity is visible in the tectorial membrane (arrow) and anterior longitudinal ligament with associated hemorrhage. The tip of the clivus (basion) is displaced anteriorly relative to the tip of the dens. Incipient spinal cord compression is apparent at the C1 level, still unaccompanied by signal changes. Blood or fluid is noted in the sphenoid sinus. (b) Sagittal T2w TSE image of the craniocervical junction. Atlantoaxial dislocation is indicated by a loss of congruence between the occipital condyle and the condylar fossa of the atlas (arrow). (c) Coronal PDw TSE image of the craniocervical junction demonstrates bony avulsions of the alar ligaments from the occipital condyles with associated hemorrhage (arrow). (d) Compare with the right alar ligament in a healthy subject. This image is angled to the course of the ligament (arrow) in an oblique coronal plane. Other important structures in this region are the alar ligaments. They connect the tip of the dens to the occipital condyles and function as restraints to head rotation, which is why they are frequently involved by impact trauma to the rotated head. These ligaments are richly endowed with receptors and neural pathways to the brainstem; this has led to comprehensive MRI studies dealing with vertigo symptoms and other chronic complaints following whiplash trauma to the neck. Appropriate thin-slice imaging protocols and slices angled along the course of the alar ligaments are essential for an accurate evaluation ( ▶ Fig. 13.3c, d). While CT can demonstrate bony avulsion injuries, MRI can detect ligament ruptures, hematomas, and edema. The definite detection of blood or ligament avulsions confirms high-energy trauma to the craniocervical junction and should prompt a detailed evaluation of the entire region including the brainstem. These injuries are also important in disability evaluations when identified during the early posttraumatic period. Pitfall Beware of overinterpreting mild edema or fatty deposits in the alar ligaments, because comprehensive studies in normal subjects have shown a high degree of variability in these structures. MRI examinations of the alar ligaments months or years after trauma for purposes of disability assessment should be performed and interpreted with extreme restraint. The criteria for evaluating positional relationships at the craniocervical junction are the same in MRI as in other imaging modalities. The interpretation of sagittal images should begin with an assessment of anterior and posterior alignment and an harmonious spinolaminar line. The tip of the clivus should be above the anterior convexity of the tip of the dens. The normal atlantodental interval measures 2.5 mm in adults and up to 4 mm in children. Values from 3 to 7 mm are reported in the literature for the maximum thickness of the prevertebral soft tissues at the level of the C2 vertebra. It should not exceed 22 mm at the level of the C6 vertebra. Of course, the advantage of MRI for this application lies in the accurate depiction of blood collections, regardless of their extent. CT is excellent for the diagnosis and classification of atlas and axis fractures. These injuries should also be diagnosed and classified with MRI, however ( ▶ Fig. 13.4, ▶ Fig. 13.5). MRI can detect ligament ruptures, especially of the anterior and posterior longitudinal ligaments, tectorial membrane, and transverse ligament. Paravertebral hematomas and ▶ spinal cord lesions are clearly visualized. This can be important in patients with dens fractures (odontoid fractures), which are divided into three types in the Anderson and D’Alonzo classification ( ▶ Fig. 13.6): Fig. 13.4 Patient with multiple injuries. (a) Axial CT clearly displays a fracture through the left side of the anterior arch of the atlas (Gehweiler I). (b) T2w MR image also demonstrates the anterior arch fracture (arrow) with an intact transverse ligament. (See also ▶ Fig. 13.5.) Fig. 13.5 Injuries of the atlas. Diagrammatic representation (source: Mutze S. Posttraumatische radiologische Diagnostik der Halswirbelsäule. Radiologie up2date 2012; 3: 231–243). (a) Fracture of the anterior arch of the atlas (Gehweiler I). (b) Fracture of the posterior arch of the atlas (Gehweiler II). (c) Fracture of the anterior and posterior arches (Gehweiler III = Jefferson four-fragment fracture). (d) Fracture of the lateral masses (Gehweiler IV). (e) Fracture of the transverse processes (Gehweiler V). (f) Jefferson fracture with two fragments. (g) Jefferson fracture with three fragments. Fig. 13.6 Anderson and D’Alonzo classification of dens fractures. I = Apical dens fracture (rare) II = Basal dens fracture III = Basal dens fracture extending into the vertebral body (Bohndorf K, Imhof H. Radiologische Diagnostik der Knochen und Gelenke. Stuttgart: Thieme; 1998; 44–53, Mutze S. Posttraumatische radiologische Diagnostik der Halswirbelsäule. Radiologie up2date 2012; 3: 231–243) Type I: This type involves the tip of the dens and is considered stable. Type II: This fracture runs through the base of the dens and is considered unstable. Type III: This fracture runs through the dens and into the lateral masses of C2. It is considered stable owing to the relatively large cancellous bone surfaces, hence it is amenable to conservative treatment. Failure of fusion of the os terminale may lead to misinterpretation, as it can mimic a dens fracture. If fusion of the dens to the body of C2 is absent or delayed, it may be misdiagnosed as a type II fracture. With a fusion anomaly, the margins of the odontoid process are usually smooth and often there is compensatory prominence of the anterior arch of the atlas. MRI can be used for differentiation in selected cases. The preferred imaging modality for fracture classification is CT. Before surgical treatment of a displaced Anderson type II fracture, the surgeon may request MRI of the spinal cord to document preoperative changes; this may be also done for medicolegal reasons. The detection of spinal cord lesions is particularly important in patients who can tolerate only a limited neurologic examination. MRI is also indicated for the evaluation of C2 arch fractures. First described as a “hangman’s fracture” in the early 1900s, this neural arch fracture of the axis caused by hyperextension and distraction can also occur in motor vehicle accidents. It accounts for approximately 7% of all cervical spine fractures. The Effendi classification ( ▶ Fig. 13.7) is used in determining the need for operative treatment. It addresses possible involvement of the C2–C3 intervertebral disk. Type I fractures are not associated with disruption of the C2–C3 disk. Type II injuries are associated with detectable disk involvement. Type III injuries are characterized by disk disruption plus uni- or bilateral dislocation of the facet joints. Types II and III fractures require surgical treatment. MRI is excellent for assessing involvement of the C2–C3 intervertebral disk. Fig. 13.7 Effendi classification of axis arch fractures. Hangman’s fracture (source: Bohndorf K, Imhof H. Radiologische Diagnostik der Knochen und Gelenke. Stuttgart: Thieme; 1998; 44–53, Mutze S. Posttraumatische radiologische Diagnostik der Halswirbelsäule. Radiologie up2date 2012; 3: 231–243). The prognosis of patients with cervical spine fractures is significantly worsened by concomitant vascular injuries. The reported prevalence of these events is 0.38 to 1.00% in the literature, although there may well be a significant percentage of unreported cases. Fractures of the atlas, axis, and lower cervical vertebrae may lead to dissecting injuries of the vertebral and internal carotid arteries in numerous combinations affecting one or both sides. The ideal examination would be contrast-enhanced CT on admission, but currently this is a realistic option only at specialized trauma centers. Color duplex ultrasound cannot reliably detect dissection-related stenosis near the skull base with less than 50% luminal narrowing. Consequently, MRI has an important role in the investigation of presumed vascular lesions, even if it is not used as an initial imaging study. The presence of suggestive fracture lines (e.g., through the transverse foramen) or fracture-dislocations, clinical signs such as Horner’s syndrome, and ischemic signs due to thromboembolic events from dissected vessels are indications for MRA; ▶ Fig. 13.8). Fig. 13.8 Fracture of the C5–C7 vertebral bodies sustained in a motor vehicle accident. Dissection of the left internal carotid artery (arrows) with marked, irregular luminal narrowing affecting a long segment of the vessel. (a) Axial arterial MRA, inflow technique. (b) MIP.
13.3 Spinal Ligament Injuries


13.3.1 Injuries of the Craniocervical Junction and Upper Cervical Spine
13.3.1.1 Atlanto-Occipital Dislocation and Subluxation

13.3.1.2 Fractures of the Atlas and Axis



13.3.1.3 Neural Arch Fractures of the Axis

13.3.1.4 Dissection of Arteries Supplying the Brain

Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


