 ▪ FIGURE 14-1 A major use of ultrasound is the acquisition and display of the acoustic properties of tissues. A transducer array (transmitter and receiver of ultrasound pulses) directs sound waves into the patient, receives the returning echoes, and converts the echo amplitudes into a 2D tomographic image using the ultrasound acquisition system. Exams requiring a high level of safety such as obstetrics are increasing the use of ultrasound in diagnostic radiology. (Photo credit: Emi Manning, UC Davis Health System.) |
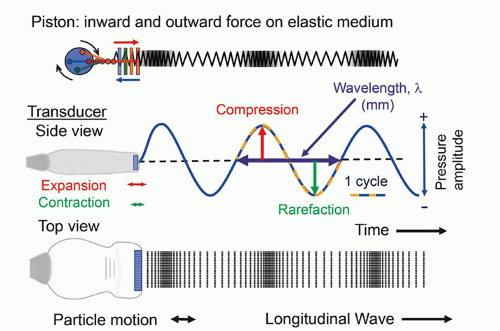 ▪ FIGURE 14-2 Ultrasound energy is generated by mechanical displacement of an elastic medium, modeled as a compressible spring. An inward and outward force of a piston coupled to the medium creates increased pressure (compression) and decreased pressure (rarefaction) in a cyclical manner (top row). Constituents (particles) of the medium transfer energy to adjacent particles with minor back and forth displacement. The ultrasound transducer is the mechanical energy source that expands and contracts like the piston at very high frequency. This results in the introduction of ultrasound into the tissues, with propagation as a longitudinal wave. The wavelength is equal to the distance of one cycle. |




TABLE 14-1 DENSITY, SPEED OF SOUND, AND ACOUSTIC IMPEDANCE FOR TISSUES AND MATERIALS RELEVANT TO MEDICAL ULTRASOUND | ||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||


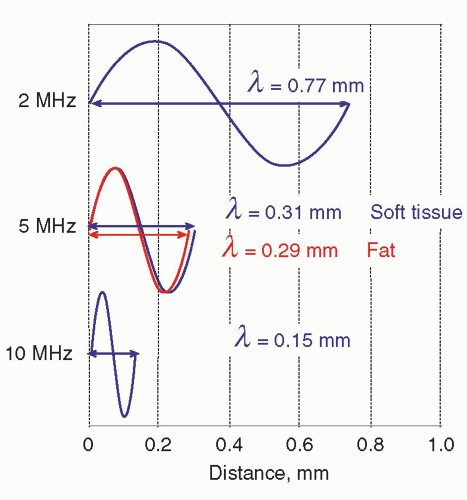 ▪ FIGURE 14-3 Ultrasound wavelength is determined by the frequency and the speed of sound in the propagation medium. Wavelengths in soft tissue are calculated for 2-, 5-, and 10-MHz ultrasound sources for soft tissue (blue). A comparison of wavelength in fat (red) to soft tissue at 5 MHz is also shown. |



manageable number range. Pressure is proportional to voltage, and Equation 14-2 is important when comparing voltages that are induced by the reception of echoes by the transducer elements (see Section 14.4). Note: when considering pressure or voltage comparisons, the dB scale is a factor of 2 higher compared to intensity comparisons, so the dB scale must be used in context. Using Equation 14-3, an intensity ratio of 106 (e.g., an incident intensity one million times greater than the returning echo intensity) is equal to 60 dB, whereas an intensity ratio of 102 is equal to 20 dB. A change of 10 in the relative intensity dB scale corresponds to an order of magnitude (10 times) change; a change of 20 corresponds to two orders of magnitude (100 times) change, and so forth. When the intensity ratio is greater than one (e.g., the incident ultrasound intensity greater than the detected echo intensity), the dB values are positive; when less than one, the dB values are negative. A loss of 3 dB (-3 dB) represents a 50% loss of signal intensity. The tissue thickness that reduces the ultrasound intensity by 3 dB is considered the “half-value” thickness (HVT). In Table 14-2, intensity ratios, logarithms, and the corresponding intensity dB values are listed.
TABLE 14-2 INTENSITY RATIO AND CORRESPONDING DECIBEL VALUES | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
in Table 14-1, right column. The efficiency of sound energy transfer from one tissue to another is largely based upon the differences in acoustic impedance—if impedances are similar, a large fraction of the incident intensity at the boundary interface will be transmitted, and if the impedances are largely different, a large fraction will be reflected. In most soft tissues, these differences are typically small, allowing for ultrasound travel to large depths in the patient.


 ▪ FIGURE 14-4 Reflection and refraction of ultrasound occur at tissue boundaries with differences in acoustic impedance, Z. A. With perpendicular incidence (90°), a fraction of the beam is transmitted, and a fraction of the beam is reflected to the source at a tissue boundary. B. With non-perpendicular incidence (≠ 90°), the reflected fraction of the beam is directed away from the transducer at an angle θr = θi. The transmitted fraction of the beam is refracted in the transmission medium at a transmitted refraction angle greater than the incident angle (θt > θi) when c2 > c1, and the refraction angle of the transmitted beam is less than that of the incident angle when c2 > c1. |
TABLE 14-3 PRESSURE AND REFLECTION COEFFICIENTS FOR VARIOUS INTERFACES | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
 . For small angles, this can be approximated as
. For small angles, this can be approximated as  . Figure 14-4B illustrates the refraction angle when the speeds of sound in tissue 1 are greater than or less than tissue 2.
. Figure 14-4B illustrates the refraction angle when the speeds of sound in tissue 1 are greater than or less than tissue 2.logarithmically to the base 10, the beam intensity is attenuated to the power of 10 with distance (See Fig. 14-6). Careful selection of the transducer frequency must be made in the context of the imaging depth needed for an exam. The loss of ultrasound intensity in decibels (dB) can be determined empirically for different tissues by measuring intensity as a function of distance traveled in centimeters (cm) and is the attenuation coefficient µ, expressed in dB/cm. For a given ultrasound frequency, tissues and fluids have widely varying attenuation coefficients chiefly resulting from structural and density differences, as indicated in Table 14-4 for a 1-MHz ultrasound beam.
 ▪ FIGURE 14-5 Specular and non-specular boundary characteristics are partially dependent on the wavelength of the incident ultrasound. For long wavelengths, tissue boundary interactions are smooth and mirror-like. As the wavelength reduces with higher frequency ultrasound, the boundary becomes “rough” with non-perpendicular surfaces that result in diffuse scattering from the surface. |
 ▪ FIGURE 14-6 Ultrasound attenuation occurs exponentially with penetration depth and increases with increased frequency. The plots are estimates of a single frequency ultrasound wave with an attenuation coefficient of (0.5 dB/cm)/MHz of ultrasound intensity versus penetration depth. Note that the total distance traveled by the ultrasound pulse and echo is twice the penetration depth. |
TABLE 14-4 ATTENUATION COEFFICIENT µ(dB/cm-MHz) FOR TISSUES ENCOUNTERED IN ULTRASOUND | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||


of mechanical strain in response to an applied electrical field. Ultrasound transducers for medical imaging applications employ a synthetic piezoelectric ceramic, lead-zirconate-titanate (PZT), or a silicon-based capacitive micromachined ultrasound transducer (CMUT).
 ▪ FIGURE 14-7 The piezoelectric element is comprised of aligned molecular dipoles. A. Under the influence of mechanical pressure from an adjacent medium (e.g., an ultrasound echo), the element thickness contracts (at the peak pressure amplitude), achieves equilibrium (with no pressure), or expands (at the peak rarefactional pressure) causing realignment of the electrical dipoles to produce positive and negative surface charge. Surface electrodes measure the amplitude of the charge in millivolt to microvolt output as a function of time in receive mode. B. An external voltage source (˜100 V) applied to the element surfaces over several microseconds causes compression or expansion from equilibrium by realignment of the dipoles in response to the electrical attraction or repulsion force in transmit mode. |
 ▪ FIGURE 14-8 A short-duration voltage spike causes the piezoelectric element to vibrate at its natural resonance frequency, f0, which is determined by the thickness of the transducer equal to ½λ. Low-frequency oscillation is produced with a thicker piezoelectric element. |
functions in an excitation mode to transmit ultrasound energy, and in a reception mode to receive ultrasound energy. To be able to use the pulse-echo format, there is a need to shorten the pulse.
 ▪ FIGURE 14-9 A. A singleelement crystal with surface electrodes, showing the thickness, width, and height dimensions. B. A section of a multielement transducer array at equilibrium (blue), thickness mode contraction (green), and expansion (red). With thickness mode variation there is also variation in the width and height of the array. The dashed double arrows represent the equilibrium dimensions. |
 , where f0 is the center frequency and the bandwidth is the width of the frequency distribution. A high “Q” transducer operation has a narrow bandwidth and a long spatial pulse width, which is good for evaluating frequency shifts such as are used in pulsed Doppler studies for measuring blood velocities (Section 14.8). A low “Q” transducer has heavy damping and a rapid ring-down of the crystal vibration to achieve a short SPL for imaging studies.
, where f0 is the center frequency and the bandwidth is the width of the frequency distribution. A high “Q” transducer operation has a narrow bandwidth and a long spatial pulse width, which is good for evaluating frequency shifts such as are used in pulsed Doppler studies for measuring blood velocities (Section 14.8). A low “Q” transducer has heavy damping and a rapid ring-down of the crystal vibration to achieve a short SPL for imaging studies. ▪ FIGURE 14-10 A. The transducer is comprised of a housing, electrical insulation, and a composite of active element layers, including the PZT crystal, damping block and absorbing material on the backside, and a matching layer on the front side of the multielement array. B. The ultrasound spatial pulse length is based upon the damping material causing a ring-down of the element vibration. For imaging, a pulse of 2 to 3 cycles is typical, with a wide frequency bandwidth, while for Doppler transducer elements, less damping provides a narrow frequency bandwidth. |
 ▪ FIGURE 14-11 Multifrequency transducer transmit and receive response to operational frequency bandwidths allows the operator to select an appropriate transmit and receive frequency depending on the type of exam, type of transducer, the transducer bandwidth range, and the need for penetration depth (selecting lower frequency) or spatial resolution (selecting higher frequency). The transducer response shown has a selectable frequency range of 4 to 10 MHz. |
 ▪ FIGURE 14-12 A. The linear array transducer activates a subgroup of transducer elements to produce an ultrasound beam directed perpendicular to the array, repeating with incremental shifting of the subgroup element by element. A rectangular field of view is produced. B. A common linear array transducer with a 6 to 15 MHz range of operation is pictured. |
can be interactively selected by the operator. The smaller physical dimension of the transducer array is useful for access to intercostal acoustic windows when performing heart and thoracic imaging exams. With a sector-scan format, the FOV dimension can be limited in regions proximal to the transducer array. A 1-5 MHz phased array transducer is shown in Figure 14-14C.
 ▪ FIGURE 14-13 A. The curvilinear (also known as convex) array operates with subgroup transducer element excitation, like the linear array. A convex arrangement produces a trapezoidal field of view, with good coverage proximally and extended coverage distally. B. A common curvilinear array transducer with a 1 to 6 MHz range of operation is pictured. |
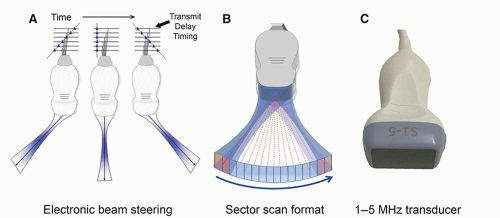 ▪ FIGURE 14-14 A. A phased array transducer produces a beam from the near simultaneous excitation of all array elements. The beam can be electronically steered across the FOV using transmit delay excitation patterns—three are shown. B. A sector scan format is produced with incremental time delay patterns to control the direction and number of lines across the FOV. C. A common phased array transducer with a 1-5 MHz range of operation is pictured. |
intraoral applications. The mechanically scanned curved array transducer is commonly used in obstetrical evaluations for 3D volume image acquisitions. Mechanical scanning of the curved array occurs simultaneously with 2D image acquisition and is synchronized to provide volumetric sampling over a ˜90° by ˜90° FOV range as a function of time. Shaded surface and volumetric rendering generate real-time 3D movies of the fetus, as discussed in Section 14.6.
 ▪ FIGURE 14-15 Intracavitary array probes exist in a variety of shapes and acquisition geometries to directly image internal organs with cavity access. A. Endovaginal curvilinear array with very wide 150° FOV and 5-9 MHz range of operation. B. Endovaginal probe using mechanically scanned curved array transducer for 3D imaging acquisitions, with 5-9 MHz range. C. Mechanically scanned curved array transducer assembly for the acquisition of 3D volumetric imaging of the fetus, with a 4-8 MHz operational range. |
largely confined to the dimensions of the active portion of the transducer surface, with the beam converging to approximately half the transducer area at the end of the near field. The near field length is dependent on the transducer area and inversely proportional to propagation wavelength, so higher transducer frequency results in an extended near field. Lateral resolution (the ability of the system to resolve objects in a direction perpendicular to the beam direction) depends on the lateral beam dimension and is best at the end of the near field for an unfocused transducer element aperture (e.g., a subgroup of linear array transducer elements fired simultaneously).
 ▪ FIGURE 14-16 A linear array transducer subgroup excitation (top) and the expanded beam profile (middle) shows the near-field and far-field characteristics of the ultrasound beam. The near field is characterized as a collimated beam, and the far field begins when the beam diverges. Point emitters (left middle) generate constructive and destructive interference patterns that cause beam collimation and large pressure amplitude variations in the near field (lower diagram). Beam divergence occurs in the far field, where pressure amplitude monotonically decreases with propagation distance. |
collimated beam that has properties like the properties of a single crystal area transducer of the same size. Thus, for a subgroup of simultaneously fired transducers in a linear array, the focal distance is a function of the transducer area (height/width) and the transducer frequency. With slight differences in excitation time for individual elements in the subgroup aperture (or full phased array), wave interactions and summations can focus the beam.
 ▪ FIGURE 14-17 Transmit and Receive focusing. A. Transmit focusing is achieved by implementing a programmable delay time (beamformer electronics) for the excitation of the individual transducer elements in a concave pattern with outer elements energized first. The individual ultrasound pulses converge to a minimum beam diameter (the focal distance) at a predictable depth in tissue. B. Dynamic receive focusing uses receive beamformer electronics to dynamically adjust delay times for processing the received echo signals. This compensates for differences in arrival time across the array as a function of time (depth of the echo) and results in phase alignment of the echo signals by all elements to achieve a good signal output as a function of time. |
 ▪ FIGURE 14-18 Side lobes and grating lobes. A. Side lobes represent ultrasound energy produced outside of the main ultrasound beam along the same beam direction caused by height and width variations of the transducer elements. B. Grating lobes represent emission of energy at large angles relative to the direction of the beam caused by the discrete nature of the multielement transducer array. At the edges of the array, energy is emitted that does not undergo interference as shown by the inset diagram. The grating lobe intensity is low relative to the intensity of the main beam or side lobes. |
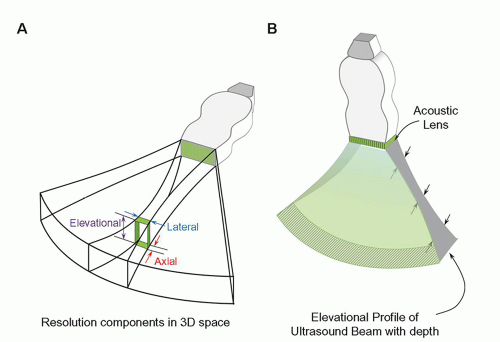 ▪ FIGURE 14-19 A. The axial, lateral, and elevational (slice-thickness) contributions in three dimensions are shown for a phased-array transducer ultrasound beam. Axial resolution, along the direction of the beam, is independent of depth; lateral resolution and elevational resolution are strongly depth dependent. Lateral resolution is determined by transmit and receive focus electronics; elevational resolution is determined by the height of the transducer elements. At the focal distance, axial is better than lateral, and lateral is better than elevational resolution. B. Elevational resolution profile with an acoustic lens across the transducer array produces a weak focal zone in the slice-thickness direction. |
 ▪ FIGURE 14-20 Axial resolution is equal to ½ SPL. Tissue boundaries that are separated by a distance greater than ½ SPL produce echoes from the first boundary that are completely distinct from echoes reflected from the second boundary, whereas boundaries with less than ½ SPL result in overlap of the returning echoes. Higher frequencies reduce the SPL and thus improve the axial resolution, as shown in the lower diagram. |
 ▪ FIGURE 14-21 Lateral resolution is a measure of the ability to discern objects perpendicular to the direction of beam travel and is determined by the beam diameter. Point targets in the beam are averaged over the effective beam diameter in the ultrasound image as a function of depth. Best lateral resolution occurs at the focal distance; good resolution occurs over the focal zone. |
resolvability for array transducers. The use of an acoustic lens across the entire array can provide improved elevational resolution at a fixed focal distance. Unfortunately, this compromises resolution before and after the elevational focal zone due to partial volume averaging.
 ▪ FIGURE 14-22 Linear and phased-array transducers have multiple user-selectable transmit and receive focal zones implemented by the beamformer electronics. In this example, a phased array transducer is illustrated. Each focal zone requires the transmit beamformer excitation of the active array for a given focal distance. Subsequent processing meshes the independently acquired data to enhance the lateral focal zone over a greater distance. Good lateral resolution over an extended depth can be achieved at the expense of reduced image frame rate. |
focusing can produce smaller slice thickness over a range of tissue depths. A disadvantage of elevational focusing is a frame rate reduction penalty required for multiple excitations to build one image. The increased width of the transducer array also limits positioning flexibility. Extension to full 2D transducer arrays with enhancements in computational power allows 3D imaging with more uniform resolution throughout the image volume.
 ▪ FIGURE 14-23 Elevational resolution with multiple transmit focusing zones is achieved with “1.5D” transducer arrays to reduce the slice-thickness profile over an extended depth. Five to seven rows of discrete arrays replace the single array. Phase delay timing provides focusing in the elevational plane, like that used for lateral transmit and receive focusing.
Related posts: X-ray Production, Tubes, and Generators X-ray Production, Tubes, and Generators
 X-ray Dosimetry in Projection Imaging and Computed Tomography X-ray Dosimetry in Projection Imaging and Computed Tomography
 Magnetic Resonance Imaging: Advanced Image Acquisition Methods, Artifacts, Spectroscopy, Quality Control, Siting, Bioeffects, and Safety Magnetic Resonance Imaging: Advanced Image Acquisition Methods, Artifacts, Spectroscopy, Quality Control, Siting, Bioeffects, and Safety
 Radiation Detection and Measurement Radiation Detection and Measurement
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|