Fig. 38.1
Understanding how to use the variety of features on a modern ultrasound machine will optimize imaging ability. A rectangular image is unable to fully encompass the width of the thyroid, whereas using the trapezoidal imaging feature of the same probe allows the entire gland to be seen
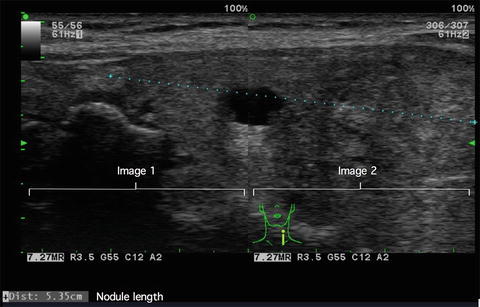
Fig. 38.2
The measurement of a large lesion may not be possible if it exceeds the width of the ultrasound probe. By “fusing” two images side-by-side, the length may be accurately measured
38.5 Optimizing the Use of Ultrasound in the Office
The vast majority of patients presenting to a surgical practice have had prior ultrasound evaluations. Findings on that study often prompted the surgical consultation. It is essential to review those prior reports and images so as to fully understand the issues to address at that consultation as well as to better hone in on what needs to be evaluated during that office ultrasound.
The patient with Hashimoto’s thyroiditis may be referred due to suspicion of multiple thyroid nodules. The prior imaging may demonstrate the measurement of multiple small lesions within the thyroid gland. Upon your ultrasound evaluation, you appreciate that on the real-time examination these findings reflect the heterogeneity within the thyroid parenchyma rather than true nodules, often called pseudonodules.
In patients with multinodular goiter, the size of purported nodules may have increased over a short period of time. Careful comparison of prior images to the real-time examination may reveal that different nodules were reported from one examination to another or, as is often the case, two adjacent nodules may be subsequently reported as one much larger nodule. Reported increase in size of the thyroid also needs to be carefully evaluated.
A patient with the length of a thyroid lobe reported as 5 cm on one examination may subsequently be reported as having increased to 6.5 cm. This may simply reflect, as the thyroid parenchyma gradually tapers out at its superior and inferior most aspect, that the placement of the measurement calipers may vary significantly. For this reason, the overall width and depth of a thyroid lobe are much more reliably followed on serial examination (Fig. 38.3).
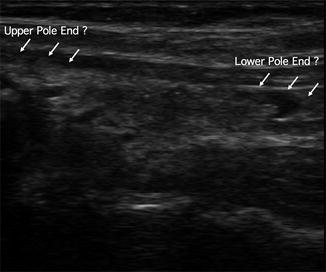
Fig. 38.3
Although the longest dimension of a thyroid lobe, the exact length may not be easily appreciated given tapering of the thyroid parenchyma . This results in potential variability on serial studies that may be misinterpreted as a true increase in size
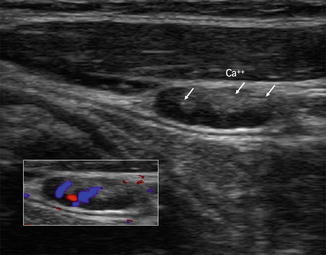
The patient referred with a worrisome thyroid nodule due to multiple “fine calcifications” many in fact be a typical benign spongiform nodule with inspissated colloid within the cystic areas mimicking calcifications. An understanding of these discrepancies will allow for an appropriate clinical decision to be made.
Patients typically come into the office very concerned that there have been untoward changes in their thyroid and are typically told that they need biopsy and/or surgery. I find it quite useful at the completion of the ultrasound examination to show the patient their findings in real time on the ultrasound screen. This provides better reassurance, typically, that intervention is not required at this point and gives them an understanding as to any discrepancy between prior imaging and the current evaluation. To reassure these patients that important findings have not been overlooked, I will typically see them back for a follow-up evaluation. To this end, it is extremely useful to have the ability to capture images into the hospitals electronic medical record. This is key for image comparison both on a follow-up office visit and in the operating room.
The technique and conduct of the ultrasound evaluation is key for extracting the maximal amount of information from the examination and arriving at the proper clinical decision. Although aware of prior examination and imaging findings, it is important to keep an open and unprejudiced frame of mind while conducting the examination. Prior documentation of a benign thyroid nodule by FNA should not dissuade careful examination of the contralateral lobe nor of lymph nodes demonstrating worrisome sonographic features. Parathyroid adenomas may occasionally be identified in patients without prior suspicion of primary hyperparathyroidism.
In performing a thyroid ultrasound, it is important to conduct the examination in a standard fashion as well as to perform image capture and annotation systematically. There is no absolute right or wrong way to form this study, but establishing a routine will guarantee that a thorough examination has been performed and that essential elements are not omitted due to attention being focused on a major finding. It is also essential to understand that although we may use the term “thyroid” ultrasound , what this means in the surgeon’s office is a comprehensive neck ultrasound. Although our initial attention may be directed at a thyroid nodule that prompted surgical consultation, careful evaluation must be performed of the contralateral lobe, potential cervical adenopathy or other unexpected anatomic findings that may be key to directing needle aspiration or indication for surgery.
I prefer to start with a transverse view centered over the thyroid isthmus. This gives me a “lay of the land” in terms of the overall thyroid appearance as well as determining whether the trachea remains in the midline. By determining the shift from the midpoint of the transducer centered over the trachea to the sternal notch, quantitative measurement of tracheal deviation is included in the ultrasound report .
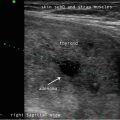
I then perform transverse imaging of one lobe with care to examine all of the central neck compartment tissue from well above to well below the limits of the thyroid parenchyma itself. This includes attention to any central neck lymph nodes. I then perform longitudinal imaging of the same region. Any thyroidal or extra thyroidal abnormalities are then assessed with color flow Doppler (Fig. 38.4).
 Ultrasound-Guided Laser Ablation
Ultrasound-Guided Laser Ablation
 Transcutaneous Laryngeal Ultrasonography: Clinical Variables
Transcutaneous Laryngeal Ultrasonography: Clinical Variables
 Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
 Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
 Feature Illustration: Vascularity
Feature Illustration: Vascularity
 Pattern Recognition: Diffuse Thyroid Disease
Pattern Recognition: Diffuse Thyroid Disease




Related posts:
Ultrasound-Guided Laser Ablation
Transcutaneous Laryngeal Ultrasonography: Clinical Variables
Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
Feature Illustration: Vascularity
Pattern Recognition: Diffuse Thyroid Disease
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
