Chapter Outline
Introduction
Soft tissue masses of the musculoskeletal system are extremely common. The vast majority of lesions are benign and in many of these cases malignancy can be excluded from the history and examination without resort to imaging.
Because of the overwhelmingly high ratio of benign to malignant lesions there is often a delay in diagnosing the latter and early imaging is therefore recommended when the nature of a mass is in doubt.
Ultrasound and MRI are the principal techniques for investigating soft tissue masses. As in other areas of musculoskeletal imaging the two techniques are complementary and both may be employed in any individual case.
In most peripheral and superficial lesions ultrasound provides all the information required.
The clinician referring a patient with a suspected soft tissue mass is usually asking one or more of the following questions: (a) is there a lesion? (b) where is it? (c) what is it? Ultrasound has been shown to be a highly sensitive technique in the detection of soft tissue masses. A normal ultrasound examination excludes a soft tissue mass with a high degree of certainty. Although not often helpful in making a precise diagnosis, ultrasound can readily differentiate solid from cystic lesions. Purely cystic lesions are benign whereas a minority of solid or mixed lesions may turn out to be malignant. Other ultrasound features such as lesion morphology, calcification, compressibility, the presence and type of vascularity and the pattern of internal echoes can all help to narrow the differential diagnosis. MRI will provide additional information with regard to tissue type in lipomatous lesions, fibrous lesions and those containing haemosiderin or other blood products. Cysts rarely require biopsy but are often subjected to ultrasound-guided aspiration. Small superficial solid lesions are suitable for excisional biopsy. Larger or deeper lesions require staging with MRI and, in most cases, preoperative biopsy, which can be performed under ultrasound control. Although ultrasound is generally nonspecific, a confident diagnosis can commonly be obtained by taking into consideration the clinical features along with the ultrasound appearances. This chapter covers the role of ultrasound in the assessment of soft tissue masses with emphasis on those conditions which exhibit specific ultrasound features.
Lipomatous Tumours
Lipomatous tumours range from the benign lipoma to highly malignant forms of liposarcoma. Well-differentiated liposarcomas do not metastasize but have the potential for local recurrence and may rarely dedifferentiate. The term ‘atypical lipoma’ is sometimes used for the lowest grade of liposarcoma to reflect the nonaggressive nature of these lesions. Lipoblastoma is a benign tumour of childhood and hibernoma is a benign tumour of brown fat. In general, benign lipoma, its variants and well-differentiated liposarcomas are seen as echogenic lesions on ultrasound in contrast to most other soft tissue tumours. Although ultrasound may be used to diagnose the simple subcutaneous lipoma, MRI is considered superior for all other lesions on account of the characteristic signal returned by fat. As deep-seated lipoma cannot be differentiated from liposarcoma, all deep lesions should be imaged by MRI prior to surgery.
Lipomatous tumours can be divided into those that are confined to the superficial fat and those that lie deep to the superficial muscle fascia. Superficial lesions are overwhelmingly benign and the vast majority of liposarcomas lie deep to the fascia.
Superficial Lipomatous Tumours
The majority of lipomas are found in subcutaneous fat. Lesions predominate in the trunk and proximal part of the limbs, the shoulder girdle region being a particularly common site for large lipoma. An ultrasound request is usually prompted by the patient noticing an increase in the size of a lesion or the discovery of a new lump. Most superficial lipomas have characteristic features on ultrasound and do not require additional imaging or biopsy.
A typical subcutaneous lipoma is an elliptical, well-defined, compressible lesion containing short linear reflective striations that run parallel to the skin surface ( Fig. 31.1 ).

| One can still make a confident diagnosis of a lipoma when there is a palpable superficial mass and no apparent underlying abnormality on ultrasound. |


Deep Lipomatous Tumours
Deep-seated lipomas are uncommon compared with their superficial counterparts and may occur in an intermuscular or intramuscular position.
Some intramuscular lipomas may have ill-defined borders due to interdigitation of fat with the muscle fibres. This feature is much better demonstrated on MRI and, when present, suggests that the lesion is at the benign end of the spectrum. Most deep lesions are best imaged with MRI. Deep-seated lipomas and atypical lipomas (previous known as well-differentiated liposarcomas) may have similar ultrasound features and MRI is therefore indicated. Although the detection of nonfatty tissue on MRI implies that the lesion is not a simple lipoma atypical lipoma may also suppress entirely on fat suppression sequences.

Nearly all liposarcomas of the extremities lie deep to the superficial muscle fascia. The term liposarcoma covers a range of tumours with varying histological and imaging features. The incidence peaks in the sixth and seventh decade and the thigh is the commonest site. Well-differentiated liposarcoma is now termed atypical lipoma; it is at the most benign end of the spectrum and is typically hyperechoic relative to adjacent muscle ( Fig. 31.5 ). The lesion has no metastatic potential and the prognosis is excellent if excision is complete. Neglected lesions will continue to grow and are at small risk of dedifferentiating into a higher grade of sarcoma. Myxoid liposarcoma contains numerous lipoblasts and small plexiform vessels in a well-vascularized myxomatous stroma that has a variable fat content. The proportion of myxoid material, lipid-containing tumour and more cellular tumour can vary, giving a spectrum of imaging appearances. Some tumours are almost purely myxoid and give very uniform homogeneous features on imaging. On MRI these lesions are usually homogeneous and, without the benefit of ultrasound or intravenous contrast, could be misinterpreted as representing a cystic lesion.
| On ultrasound myxoid liposarcoma may resemble a cyst, being uniformly hypoechoic, but on careful examination the internal structure can be detected and internal vascularity can usually be detected. |
Biopsy of lipomatous tumours rarely influences management and can be safely omitted in most cases.


Other Benign Lipomatous Tumours
There are several lipoma variants. Angiolipomas are probably hamartomatous lesions. They typically present as a small, sometimes painful, superficial mass in the young adult. They are most commonly encountered in subcutaneous fat of the arms and chest and are often multiple. On ultrasound they are seen as small hyperechoic masses with variable vascularity. Fibrolipoma describes a lipoma with abundant fibrous strands. The lesions are hyperechoic and cannot be distinguished from simple lipomas. Lipoblastoma is a rare tumour of childhood, usually seen under the age of 3 years. The tumour is typically lobulated, may contain cystic areas and is hypovascular. Fat signal may or may not be seen on MRI or CT. On ultrasound the lesion has been described as uniformly echogenic and generally hypovascular, although small amounts of flow may be seen on Doppler. Hibernoma is a benign tumour of brown fat. It occurs chiefly in the upper thorax in patients in their fourth and fifth decade. Clinically it behaves in a manner similar to that of simple lipomas. On MR the signal intensity of the lesion is less high on T1-weighted images than that of lipoma, reflecting the smaller proportion of fat-containing cells. Hibernomas are more vascular than lipomas and will enhance following contrast. The ultrasound appearances have been described as showing a hyperechoic, vascular mass.
Muscle Tumours
Primary tumours of the muscle are rarely encountered in the musculoskeletal system. Ultrasound features are generally nonspecific. Ultrasound is useful in diagnosing accessory muscles and muscle hernias, both of which may present as a mass. Leiomyomas are rare and are usually small cutaneous lesions that do not require imaging. Larger and deeper hypervascular lesions, which may contain calcification, are encountered. Leiomyosarcomas may be seen in the subcutaneous tissue or in muscle. They probably arise from vessel walls. Appearances are nonspecific and cannot be differentiated from other aggressive lesions. Central necrosis is a common finding on ultrasound of intraabdominal lesions. Angioleiomyoma is a relatively common superficial painful benign lesion that is very vascular and therefore may be confused with a haemangioma on ultrasound. It occurs primarily in middle age and is twice as common in females. On ultrasound the lesion appears as a well-defined hypoechoic, hypervascular mass. Rhabdomyomas are exceedingly rare and in adults occur in the neck region.
Rhabdomyosarcoma is a tumour of childhood and young adults and, although not uncommon, is rarely seen outside the abdominal cavity and pelvis or head and neck region.
Muscle Hernias and Accessory Muscle
A fascial defect may allow herniation of muscle, which may only be palpable on contraction of the muscle or, in the lower limb, on standing.

Fibrous Tumours
There are three main types of tumours of fibrous origin: benign focal fibrous tumours, diffuse fibromatous lesions (fibromatoses) and malignant fibrous lesions. In general fibrous lesions are hypoechoic lesions on ultrasound.
Benign Focal Lesions
Fibroma
In the musculoskeletal system, fibromas predominately arise from the tendon sheaths of the fingers or thumbs. The lesion affects young and middle-aged adults, predominantly men. It is not known whether the lesion represents a neoplasic or reactive process. On ultrasound a fibroma appears as a well-defined hypoechoic mass closely related to the tendon. Differentiating fibroma from a giant cell tumour is impossible on ultrasound. On MRI the two lesions may also have similar appearance, as fibrous tissue, seen in fibromas, and haemosiderin, seen in giant cell tumours, are both detected as low-signal on T2-weighted images.
Fibromatosis
Palmar and Plantar Fibromatoses
These two conditions result from fibrous proliferation of the fascia. The condition may be bilateral and the plantar and palmar versions may occur in the same patient. In the hand the patient may first notice a single nodule in the palm. Progression is slow and unpredictable. Fibrous cords extend from the lesion to the fingers, giving the characteristic feature of Dupuytren’s disease. Imaging is rarely required. In the plantar version, the patient may present with a lump, pain or both. The nodules may be solitary, multiple and situated either medially or centrally within the fascia. Unlike Dupuytren’s disease the clinical features are less specific and imaging is useful to confirm the relationship of the lesion to the plantar fascia. On ultrasound a typical plantar fibroma is seen as an elongated hypoechoic, nonvascular lesion, which blends into the fascia ( Fig. 31.8 ). A mixed echo pattern can be seen in those lesions larger than 1 cm in length. There is usually no or minimal flow detected on Doppler but the lesion can be vascular ( Fig. 31.9 ).
MRI will confirm the fibrous nature of plantar fibroma but is rarely required as the ultrasound appearances are highly specific.


Nodular Fasciitis
This is a relatively common reactive lesion of unknown aetiology seen predominantly in young adults. The patient presents with a rapidly growing solitary lump and some tenderness. The lesion is usually situated in the subcutaneous tissue but can occur in the intramuscular or intermuscular positions. The lesion involves the upper limb in about half the cases. Although the disease is self-limiting, most lesions are excised on account of the alarming growth rate. Histologically the lesion consists of immature fibroblasts in a myxoid matrix. In the few reports in the literature the lesions have been described as well defined and mixed echogenicity. The lesions do not enhance on MR or CT following intravenous contrast.
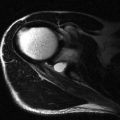
Elastofibroma
Elastofibroma is a benign tumour of unknown aetiology consisting of fibroblasts, collagen and thickened elastic fibres interspersed by fat. It is thought to be a reactive lesion rather than a neoplasm. By far the commonest site is between the chest wall and the scapula. The condition may be bilateral. On ultrasound the lesion may have a nonspecific internal echo pattern, but usually the typical linear or curvilinear hypoechoic strands against an echogenic background are seen, reflecting the interspersed fatty and fibroelastic components ( Fig. 31.10 ).