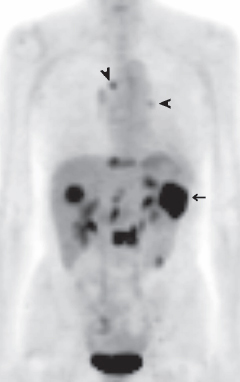
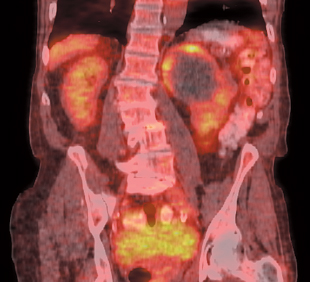
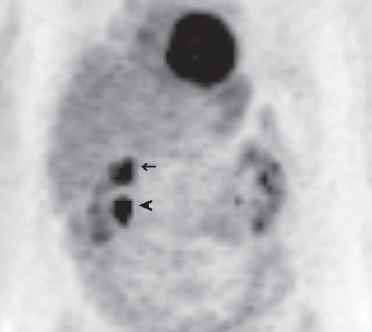
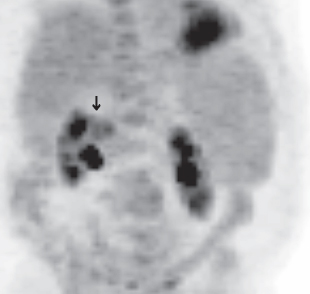
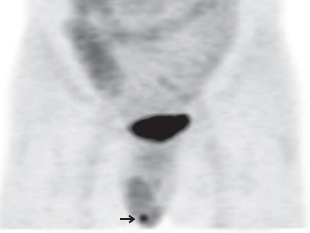
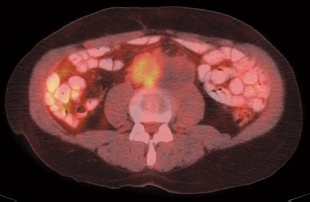
23 The role of positron emission tomography (PET) in the evaluation of renal masses is somewhat limited. Both solid and cystic renal masses can be evaluated. Renal masses are sometimes detected incidentally on PET images. FDG PET is specific for the diagnosis of malignancy in renal masses, but sensitivity will vary depending upon lesion size and location (Table 23.1). Fig. 23.1 Cystic renal cell carcinoma. Coronal positron emission tomography/computed tomography demonstrates focal areas of peripheral uptake in a large left upper pole renal cyst, consistent with cystic renal cell carcinoma. However, the lack of fluorodeoxyglucose in a complex renal cyst would not exclude renal cell carcinoma. Fig. 23.2 Renal mass or collecting system? Coronal positron emission tomography scan demonstrates focal activity in the upper pole of the right kidney (arrow). Note the similarity of appearance to renal collecting system activity (arrowhead). In this case, it is difficult to determine whether this is uptake in a renal mass or stasis in the upper pole collecting system. The uptake was secondary to a renal cell carcinoma. Fig. 23.3 Subtle renal cell carcinoma. Coronal positron emission tomography scan demonstrates a subtle medial right upper pole renal mass (arrow). Note that this is only slightly more intense than normal renal parenchyma and can only be diagnosed by the contour deformity. Most renal cell carcinomas are more intense than this. Given the relatively low sensitivity, a negative PET scan does not exclude the presence of disease for either staging or restaging purposes. The accuracy of PET in detected testicular neoplasms is unknown, but PET can sometimes detect unsuspected testicular neoplasms (Fig. 23.5). PET is valuable in staging stage II testicular germ cell tumors (Fig. 23.6), but may not be of additional value in patients with stage I tumors.12 Fig. 23.5 Testicular tumor. Focal testicular uptake is noted (arrow) on a coronal positron emission tomography scan. This was an incidentally detected right testicular seminoma. PET is useful in evaluating tumor recurrence in both seminomas and nonseminomatous germ cell tumors (NSGCT), although it is more useful in seminomas. Fig. 23.7 Seminoma with retroperitoneal mass. Axial positron emission tomography/computed tomography in a patient with seminoma demonstrates a large retroperitoneal mass. The right aspect has fluorodeoxyglucose (FDG) uptake consistent with tumor; the left aspect is cystic-appearing without FDG uptake.
Urologic Tumors
Eugene C. Lin and Abass Alavi
 Renal Cell Carcinoma:1 Renal Masses
Renal Cell Carcinoma:1 Renal Masses
Clinical Indication: C
Accuracy and Comparison with Other Modalities5
Pearls and Pitfalls
Sensitivity %
Specificity %
PET
60
100
CT
92
100
Staging and Restaging
Clinical Indication: C
Accuracy and Comparison with Other Modalities
Pitfalls
 Testicular Cancer
Testicular Cancer
Staging
Clinical Indication: C
Accuracy and Comparison with Other Modalities
Pitfalls
Recurrence
Clinical Indication: B
Sensitivity %
Specificity %
PET
80
100
CT
70
74
Accuracy and Comparison with Other Modalities
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine