Fig. 1
DXA scan results at the hip in a 67-year-old woman with a history of proximal humerus fracture. The femoral neck T-score is −2.3. The FRAX results are shown on the DXA printout just below the BMD results. Ten-year fracture risk is 3.6 % for hip fracture and 19 % for major osteoporotic fracture
A screenshot of the FRAX website is shown in Fig. 2. First, the user selects the country where the patient lives. This data is important because fracture rates and life expectancy vary significantly in different countries (Kanis et al. 2002). The current version of FRAX is available for 39 countries including China, Japan, Philippines, South Korea, Singapore, Taiwan, Austria, Belgium, Czech Republic, Denmark, Finland, France, Germany, Hungary, Italy, Malta, Netherlands, Norway, Poland, Romania, Russia, Slovakia, Sri Lanka, Spain, Sweden, Switzerland, Turkey, United Kingdom, Jordan, Lebanon, Tunisia, Canada, United Sates, Argentina, Columbia, Ecuador, Mexico, Australia, and New Zealand. If a particular country is not included in FRAX, a similar country should be selected for the analysis. In the United States, the user then selects one of the four subgroups: Caucasian, Black, Hispanic, or Asian.
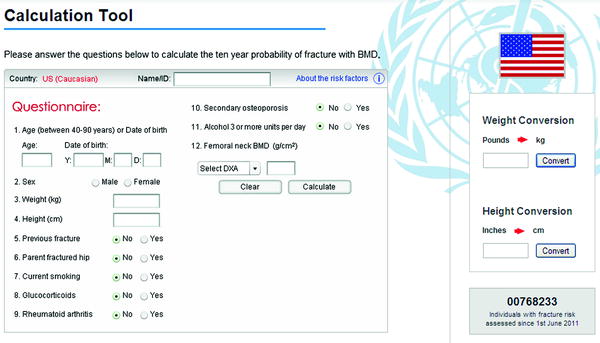
Fig. 2
FRAX Calculation tool website. The United States database is selected. The questionnaire includes: age, gender, weight, height, previous fracture, parental hip fracture, current smoking, use of glucocorticoids, rheumatoid arthritis, secondary osteoporosis, alcohol intake, femoral neck BMD
The user then answers the following questions about the patient: age, gender, weight, height, previous fracture, parental hip fracture, current smoking, use of glucocorticoids, rheumatoid arthritis (RA), secondary osteoporosis, and alcohol intake of 3 units or more daily.
Finally, the user enters the femoral neck BMD in g/cm² and selects the manufacturer of the DXA device used to measure the BMD. In settings where BMD measurement is not available, FRAX may be used to calculate fracture risk without BMD input.
Based on the provided data, FRAX calculates a 10-year probability of experiencing a hip fracture and a 10-year probability of experiencing what it terms, “major osteoporotic fracture.” Major osteoporotic fracture includes fractures involving the proximal femur, spine, proximal humerus, or distal radius.
3 Risk Factors Included in FRAX
Although BMD is an important factor in the assessment of osteoporotic fracture risk; it is not the only factor. In fact, nearly half of low-trauma fractures occur in non-osteoporotic individuals (Wainwright et al. 2005). Many clinical factors have been recognized as increasing the risk for fracture, independent of BMD. FRAX incorporates many of these risk factors in its algorithm, and it accounts for interactions between various risk factors (Kanis et al. 2007). FRAX, however, does not utilize every risk factor. For example, uncommon risk factors are excluded. Additionally, some common risk factors such as high bone turnover do not have sufficient data to be included in fracture prediction models. Some risk factors such as frailty and high frequency of falls are not easily measured. Some risk factors do not contribute to fracture risk independent of BMD. FRAX uses only those risk factors that are common, easily measurable, and have been proven in large epidemiological trials to predict fracture risk, independent of BMD.
3.1 Age
FRAX includes a question about the patient’s date of birth. It is well established that age and BMD are not only the two most powerful predictors of fracture risk, but are also partially independent predictors of that risk (Siris et al. 2006).
3.2 Gender
FRAX includes a question about the patient’s gender. It is well established that gender is an important determinate of fracture risk (Baron et al. 1996). The lifetime risk of a 50-year-old woman developing an osteoporotic fracture is approximately 50 %. The risk for the same age man is 20–30 %. It is important to recognize that despite the higher risk of fractures in women, nearly one-third of hip fractures occur in men (Eastell et al. 1998).
3.3 Height and Weight
The FRAX questionnaire includes the patient’s height and weight. Individuals with low body mass index (BMI) are at an increased risk of fracture (De Laet et al. 2005; Felson et al. 1993). Importantly, decreasing BMI over time may contribute more to fracture risk than low BMI at a given time point (Cummings et al. 1995). In the Study of Osteoporotic Fractures, women who lost 10 % of their body weight since age 25 had a hip fracture rate of 15 per 1,000 patient-years, while those who gained more than 50 % of their body weight had a rate of 1.1 per 1,000 patient-years (Cummings et al. 1995).
3.4 Previous Fracture
FRAX includes a yes or no question about the patient’s history of prior fracture. A previous fracture is defined as a spontaneous fracture in adult life or a traumatic fracture that would not normally occur in a healthy individual. Importantly, radiographic or clinical vertebral fractures may be used when answering this question.
There is abundant evidence that prior fracture is a risk factor for future fractures, independent of BMD (Center et al. 2007; Ettinger et al. 2003; Lindsay et al. 2001; Kanis et al. 2004a, b, c; Klotzbuecher et al. 2000; Schousboe et al. 2006). In a meta-analysis of peri- and postmenopausal women, fracture risk was doubled in women who had a prior fracture compared to those who had no prior fracture (Klotzbuecher et al. 2000).
3.5 Parental Hip Fracture
FRAX asks if the patient’s parent had a history of hip fracture. The question requires a yes or no response. There is evidence that fractures in parents increase the risk of fractures in the offspring. In the Study of Osteoporotic Fractures, women with a maternal history of hip fracture had twice the fracture risk compared to women without maternal history (Cummings et al. 1995). In a large meta-analysis Kanis et al. (2004a, b, c) reported that men and women with a parental history of fracture had an increased risk of any fracture (relative risk = 1.17), osteoporotic fracture (relative risk = 1.18), and hip fracture (relative risk = 1.49).
3.6 Smoking
3.7 Glucocorticoids
FRAX includes a yes or no question about patient’s use of glucocorticoids. The question should be answered yes if there is present or past oral glucocorticoid therapy for more than three months and equivalent to at least 5 mg of prednisone per day.
Glucocorticoids are associated with an increased risk of fracture (van Staa et al. 2002, 2003; Weinstein 2011). In a study of 244,235 oral corticosteroid users and 244,235 controls, relative rates of non-vertebral fractures during treatment were 1.33 and hip fractures 1.61 (van Staa et al. 2000a, b).
The use of glucocorticoids as risk factor for fracture is inversely related to the patient’s age. In a meta-analysis, Kanis et al. (2004a, b, c) reported that in 50-year olds, the relative risk of osteoporotic fractures was 2.63 and hip fractures was 4.42. In the same meta-analysis, in 80-year olds, the relative risk of osteoporotic fractures was 1.71 and hip fractures was 2.48. Importantly, the effect of glucocorticoids is independent of BMD.
3.8 Rheumatoid Arthritis
FRAX includes a yes or no question about RA. The etiology of fractures in patients with RA is multifactorial, resulting from chronic inflammation, inactivity, increased fall risk, and use of glucocorticoids (Broy and Tanner 2011). However, the increased fracture risk appears to be independent of the use of glucocorticoids.
3.9 Secondary Osteoporosis
FRAX asks if the patient has secondary osteoporosis. The question requires a yes or no response. Conditions associated with secondary osteoporosis include Type I diabetes, untreated long-standing hyperthyroidism, overtreated hypothyroidism, hypogonadism, premature menopause (<45 years), anorexia nervosa, certain breast cancer chemotherapeutic agents, hypopituitarism, inflammatory bowel disease, organ transplantation, COPD, chronic liver disease, chronic malnutrition, osteogenesis imperfecta, or prolonged immobility in conditions such as spinal cord injury, Parkinson’s disease, stroke, or muscular dystrophy (Kanis et al. 2008a, b, c).
Although most of these conditions are associated with low BMD, the association with fractures risk is less certain. It is important to recognize that in FRAX there is no increased fracture risk attributed to secondary osteoporosis if the BMD value is entered. The only exception is RA, which is a separate question in FRAX.
3.10 Alcohol Use
FRAX asks if the patient drinks three or more units of alcohol per day. The question requires a yes or no response.
The association between alcohol use and risk of fracture has not been consistent across studies (Berg et al. 2008; Høidrup et al. 1999; Kanis et al. 2005a, b, c; Mukamal et al. 2007). In one large study (Kanis et al. 2005a, b, c) intake above two units daily was associated with an increased relative risk of any fracture (RR = 1.23), osteoporotic fracture (RR = 1.38), and hip fracture (RR = 1.68). Importantly, this elevated fracture risk was independent of BMD.
3.11 Bone Mineral Density
When available, femoral neck BMD measured by DXA should be included in FRAX. The association between low BMD and an increased risk of fracture has been well established (Cranney et al. 2007; Cummings et al. 1993; Marshall et al. 1996). Importantly, the combination of BMD with clinical factors has been shown to improve risk prediction, compared to BMD or clinical risk factors alone (Kanis et al. 2007, 2012). This combination is what makes FRAX such a powerful clinical tool.
4 Various Ways to Use FRAX
In 1994, when the World Health Organization (WHO) first used BMD to define osteoporosis, the definition was intended mainly as a research tool for epidemiologists. Soon after, T-scores emerged and revolutionized the care of patients being evaluated for osteoporosis. In contrast, the introduction of FRAX by the WHO in 2008 was intended for clinical use rather than research. For this reason, various professional organizations developed guidelines for the use of FRAX in managing patients. What emerged is an approach to FRAX that is somewhat different in different countries. In particular, clinicians in the United States and the United Kingdom have chosen distinct approaches to the use of FRAX.
4.1 Indications for FRAX
In the United States, the National Osteoporosis Foundation (NOF) recommends using FRAX in postmenopausal women and in men age 50 and older. The NOF does not recommend FRAX in patients who are receiving pharmacologic therapy (NOF 2010).
In the United Kingdom, the National Osteoporosis Guideline Group (NOGG) recommends using FRAX in postmenopausal women and men over 50 years of age. However, unlike the NOF, the NOGG recommends initial use of FRAX without BMD. So in fact, FRAX results are used to determine what patients are candidates for BMD measurement using DXA. Based on age-specific thresholds of FRAX-derived risk of major osteoporotic fracture, patients are divided into three categories: (1) high risk–consider treatment, (2) intermediate risk–measure BMD, and (3) low risk–no treatment (NOGG 2010). The individuals that fall into the second group (intermediate risk) have their BMD measured and have a second FRAX calculation, this time with BMD. Based on FRAX-derived risk of major osteoporotic fracture, these patients are divided into two categories: (1) high risk–consider treatment, (2) low risk–no treatment (NOGG 2010).
In summary, in the UK, FRAX is used to select patients for DXA. In other words, every patient with DXA will have FRAX first. In contrast, in the US, DXA is used to select patients for FRAX. Based on the recommendations of the NOF and the International Society for Clinical Densitometry (ISCD), only patients with osteopenic BMD (T-score between −1.0 and −2.5) by DXA should have a FRAX calculation.
Importantly, FRAX does not provide treatment guidelines. As the indications for FRAX differ among individual countries, treatment recommendations based on FRAX are also different in various countries.
4.2 Treatment Recommendations Based on FRAX
FRAX has changed how men and women suspected of having osteoporosis are selected for pharmacologic therapy. Prior to FRAX, many guidelines relied on BMD results (T-score) for treatment recommendations. After FRAX became available, these guidelines were revised to recommend therapy in individuals who are at high risk for fracture based on FRAX. Thresholds for therapy vary by country.
In the United Sates, the NOF recommends pharmacologic intervention in men and women with osteopenia (T-score between −1.0 and −2.5 at the femoral neck or spine) and a 10-year probability of a hip fracture ≥3 % or a 10-year probability of a major osteoporosis-related fracture ≥20 % (NOF 2010). The NOF also recommends treatment in individuals with osteoporosis (T-score ≤−2.5 at the femoral neck or spine) and in individuals with a hip or vertebral (clinical or radiologic) fracture (NOF 2010).
Prior to FRAX, a 70-year-old Caucasian woman in the United States with a BMI of 19, a T-score of −1.4, and a maternal history of hip fracture would not qualify for treatment. Using FRAX, the same woman has a 10 % probability of a hip fracture and 22 % probability of a major osteoporotic fracture and would qualify for therapy based on NOF guidelines.
In the United Kingdom, the NOGG algorithm stratifies patients into low, intermediate, and high risk categories based on FRAX without BMD. High risk individuals can be considered for treatment without BMD testing. Intermediate risk individuals have DXA with FRAX. Intervention thresholds are set by age and are equivalent to the risk associated with a prior fracture for a person of that age (NOGG 2010). Like the NOF, the NOGG recommends that women with a prior fragility fracture should be considered for treatment, without the need for BMD testing.
In summary, the FRAX treatment thresholds in the UK vary by age, whereas in the US the FRAX treatment thresholds of 3 and 20 % are used for all postmenopausal women and men age 50 and older. The economic modeling that underlies these two approaches is also quite different.
4.3 Economic Modeling
FRAX-based treatment thresholds vary by country. Treatment thresholds are determined in part by country-specific economic analysis which includes costs associated with fractures and costs associated with pharmacologic therapy (Borgström et al. 2006; Burge et al. 2007; Kanis et al. 2008a, b, c).
In the United States, a cost-benefit analysis with the following assumptions was used: bisphosphonate therapy for 5 years ($600/year), yearly doctor visit ($49/year), BMD in year 2 ($82), fracture risk reduction of 35 %, and willingness-to-pay threshold of $60,000 per quality-adjusted-life-year (QUALY) gained (Tosteson et al. 2008). Osteoporosis treatment was cost-effective when 10-year hip fracture rates reached 3 %.
In the United Kingdom, a cost-benefit analysis with a different set of assumptions was used (Kanis et al. 2008a, b, c, 2009). The intervention threshold was set to coincide with the fracture probability of someone with a prior osteoporotic fracture. The cost of generic aldendronate was set at ₤95 a year. Unlike the NOF thresholds, the NOGG thresholds vary by age. For example, in a 50-year-old, a 7.5 % probability of major fracture is used; in an 80-year-old, a 30 % probability is used.
In the future, the treatment thresholds based on FRAX are expected to change based on changing drug costs, drug effectiveness, and health economics within a given country.
5 How We Use FRAX
We include FRAX in our DXA reports only in patients with DXA measured T-score between −1 and −2.5, who are older than age 50, and who are not currently being treated for osteoporosis. We do not include FRAX in our DXA reports in patients with normal or osteoporotic BMD, in non-steroid-treated patients younger than age 50, or in patients undergoing pharmacotherapy. As such, our practice is consistent with the recommendations of the NOF and ISCD.
To understand how we use FRAX, it is important to review how we use DXA (Dasher et al. 2010). Figure 3 shows our DXA report template. In the vast majority of our patients, we use our DXA interpretation to help answer three clinical questions: (1) what is the patient’s diagnosis based on BMD, (2) what is the patient’s prognosis or risk of fracture, (3) could the patient benefit from pharmacologic therapy.
Fig. 3
Our DXA report template. Note that the report is organized into sections including clinical history, BMD Results, Conclusions, and additional information. The conclusion section includes statements about diagnosis, fracture risk, monitoring, treatment recommendations, and follow-up. When appropriate, we include FRAX results in the fracture risk portion of our conclusion
The second question was always the most problematic because there are different ways to express fracture risk. For example, we could state qualitatively that the risk is increased or we could state quantitatively that the risk has a certain number. Quantitative risk, in turn, could be expressed as relative risk or absolute risk. While relative risk compares two groups, absolute risk evaluates just one group, typically over 1 year, 5 years, or 10 years. In that sense, FRAX provides an absolute risk of fracture over 10 years. Thus, when combined with DXA-measured BMD, FRAX has proven to be extremely valuable for determining a patient’s prognosis.
FRAX can also address the third clinical question by helping to select osteopenic patients for pharmacologic therapy.
In order to further emphasize the utility of FRAX in the interpretation of clinical DXA examinations, we contrast our current approach with our approach before FRAX became available.
5.1 DXA Interpretation Before FRAX
Figure 4 shows one of our typical DXA reports prior to the use of FRAX. This was a 64-year-old woman with a history of distal radius fracture. Because her BMD was in the osteopenic range (femoral neck T-score = −1.7) the fracture risk in our DXA report was expressed qualitatively as “increased.” Although at one time we used a quantitative expression of relative risk in our DXA reports, this practice was not standardized. Statements such as, “this patient’s risk is increased four-fold” were found to be confusing to many of our referring clinicians and thus were consequently abanoned. Prior to FRAX, there was no accepted way to express absolute fracture risk in DXA reports. Before FRAX, the NOF recommended therapy in patients with T-scores below −1.5 if they had clinical risk factors. Because the patient in Fig. 4 met the above NOF criteria, our DXA report included a statement, “Therapy should be considered.”
Fig. 4
Our DXA report prior to the use of FRAX. This is a 64-year-old woman with previous distal radius fracture. L1–L4 T-score of −1.1 and femoral neck T-score of −1.7. Note that the risk is expressed in qualitative terms as “increased”
5.2 Current DXA Interpretation
Figure 5 shows one of our typical DXA reports with the use of FRAX. Note that this 66-year-old woman with prior history of distal radius fracture and a femoral neck T-score of −1.5 is similar to the patient in Fig. 4. Because the patient has osteopenic BMD, the fracture risk was calculated using FRAX. However, unlike the patient in Fig. 4, this patient did not qualify for pharmacologic therapy. With a 10-year risk of hip fracture of 1.5 % and major osteoporotic fracture of 14 %, the patient did not meet the post-FRAX criteria for therapy from the NOF.
Fig. 5
a Hip DXA printout in a 66-year-old woman with previous distal radius fracture. L1–L4 T-score (not shown) is −0.8. Femoral neck T-score is −1.5. Note that the FRAX results are shown because the patient is osteopenic. b DXA report in the same patient. Note that the risk is expressed in quantitative terms based on FRAX: 10-year fracture risk is 1.5 % for hip fracture and 14 % for major osteoportic fracture. Because the patient does not meet the NOF criteria for therapy, therapy was not recommended
Figure 6 shows our use of FRAX in a DXA report of another patient, a 78-year-old woman with a history of low-trauma tibia fracture. Like the patient in Fig. 5, this patient has osteopenic BMD (femoral neck T-score is −2.0). Unlike the patient in Fig. 5, this patient met the post-FRAX criteria for pharmacologic therapy from the NOF. The 10-year risk was 5.1 % for hip fracture and 21 % for major osteoporotic fracture.
Fig. 6




a Hip DXA printout in a 78-year-old woman with previous low-trauma tibia fracture. L1–L4 T-score (not shown) is −2.2. Femoral neck T-score is −2.0. Note that the FRAX results are shown because the patient is osteopenic. b DXA report in the same patient. Note that the risk is expressed in quantitative terms based on FRAX: 10-year fracture risk is 5.1 % for hip fracture and 21 % for major osteoportic fracture. Because the patient meets the NOF criteria for therapy, therapy was recommended
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
