Abdominal Aorta
The abdominal aorta continues from the thoracic aorta as it passes posterior to the median arcuate ligament and between the crura of the diaphragm (aortic hiatus), in front of the body of the T12 vertebra and then descends slightly to the left of midline. Clinically, the abdominal aorta is often divided into suprarenal and infrarenal arterial segments. The rationale for this division is the higher incidence of atherosclerotic and aneurysmal disease in the infrarenal abdominal aorta and the increased complexity of interventions involving the suprarenal portion. It terminates as a bifurcation into two common iliac arteries anterior to the fourth lumbar vertebra.
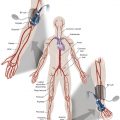
As the aorta descends through the abdominal cavity, the infrarenal aorta gives off anterior, lateral, and posterior branches. Anterior branches include the celiac trunk, superior mesenteric artery, and inferior mesenteric artery, which supply the gastrointestinal viscera, as well as the phrenic and gonadal arteries ( Fig. 19.1 ).

The bilateral inferior phrenic arteries may arise together as a trunk or as independent vessels just above or at the origin of the celiac trunk. They pass upward from the abdominal aorta to the diaphragm and give off multiple branches to the adrenal glands. The inferior phrenic artery also supplies the Glisson capsule of the liver through anastomoses at the bare area of the liver within the triangular ligaments.
The celiac trunk arises just below the aortic hiatus. A search for its origin at angiography should begin from the left pedicle of the T12 vertebra to the superior endplate of the L1 vertebra. Asymptomatic narrowing or occlusion of the origin of the celiac trunk should be anticipated by thorough review of any preprocedural imaging. It is the major supply to the foregut (liver, gallbladder, pancreas, stomach, lower esophagus) and spleen ( Fig. 19.2 ).

Celiac Trunk Variations
Classic celiac trunk anatomy is present in up to only 70% of individuals; a wide range of variants may exist. Couinaud described eight different types of variations of the celiac trunk ( Fig. 19.3 ). Type 1 involves a classic configuration of the celiac trunk, with all three branches arising as a trunk from the abdominal aorta. The variation exists in the possible subtypes: a hepatosplenic trunk, with the left gastric artery arising from the trunk; a hepatogastrosplenic trunk, with the three arteries arising simultaneously in a trifurcation; or a gastrosplenic trunk, in which the splenic artery is dominant and the hepatic artery arises from the splenic artery. Another variant described involves a common trunk for two arteries, the hepatic and splenic arteries for type 2 and the hepatic and left gastric arteries for type 3, whereas the third artery, the left gastric artery in type 2 and the splenic artery in type 3, arises directly from the aorta. Alternatively, the splenic artery in type 3 may arise from the superior mesenteric artery. Similar to a type 2 variant is type 4, in which the left gastric artery arises directly from the aorta; however, the common trunk comprises the hepatic, splenic, and superior mesenteric arteries. The most complex configuration is type 5, in which the left gastric and splenic arteries form a common trunk, and the common hepatic artery, when present, may arise from the aorta or superior mesenteric artery. When the hepatic artery does not exist, it is replaced by the right, left, or both hepatic arteries at the same time. Types 6 and 7 involve additional arteries arising from the celiac trunk, including the superior mesenteric artery in type 6 and the left colic or middle colic arteries in type 7. Additionally, the three main arteries may arise directly from the aorta, as in type 8.

The common hepatic artery, a medium-sized branch of the celiac trunk, is directed forward and to the right and divides into its two terminal branches, the hepatic artery proper and the gastroduodenal artery. The hepatic artery proper ascends toward the liver in the free edge of the lesser omentum. It runs to the left of the bile duct and anterior to the portal vein to the porta hepatis, where it divides into the right and left hepatic arteries. Prior to reaching the porta hepatis, it gives off the cystic artery to supply the gallbladder. Alternatively, the cystic artery may arise from the common hepatic, left hepatic, or even the superior mesenteric artery. Additionally, there may be more than one cystic artery. The right gastric artery arises from any site along the hepatic artery, before or after the gastroduodenal artery. It descends to the pyloric end of the stomach, passes to the left along its lesser curvature, and anastomoses with the left gastric artery.
Multiple collateral arterial pathways to the liver can occur in the event of occlusion, an important consideration during embolization of intrahepatic bleeding.
Hepatic Artery Variations
In general, 45% of patients have some variation in their hepatic arterial supply. Eight different types of variations have been described ( Fig. 19.4 ). The most common variation is the replacement of either the right hepatic artery from the superior mesenteric artery (type 3, Fig. 19.5 ) or the left hepatic artery from the left gastric artery (type 4, Fig 19.6 ). Other replaced variants include the common hepatic artery from the superior mesenteric artery (type 1). Accessory variants include an accessory right hepatic artery from the superior mesenteric artery (type 5) and an accessory left hepatic artery from either the left gastric artery (type 6) or the right hepatic artery (type 7). A type 2 variant involves early bifurcation of a short common hepatic artery or separate origins of the right and left hepatic arteries from the celiac trunk, with the gastroduodenal artery arising from the right hepatic artery. Additionally, variant anatomy may involve the pathway of the artery, with a type 8 variant involving the right hepatic artery passing anterior to the common hepatic duct instead of posteriorly. These variants can occur in isolation or together.



The gastroduodenal artery is a short but large branch of the common hepatic artery that descends near the pylorus between the superior part of the duodenum and the pancreatic neck. Together with the superior pancreaticoduodenal artery, it provides an important collateral pathway from the superior mesenteric artery in the event of celiac trunk occlusion. (See Chapter 25 for further discussion of the gastroduodenal artery.)
The superior mesenteric artery is the anterior branch of the abdominal aorta supplying the midgut, which includes the entire small bowel from the duodenum inferior to its major duodenal papilla, the cecum, the appendix, the ascending colon, and the right two-thirds of the transverse colon. At angiography, its origin should be searched for in the midline overlying the L1 vertebra, passing anteriorly and slightly to the right. (See Chapter 25 for further discussion of the superior mesenteric artery and its branches.)
The inferior mesenteric artery supplies the hindgut, which includes the left third of the transverse colon, the descending colon, the sigmoid colon, the rectum, and the upper part of the anal canal. It is the smallest of the three anterior branches of the abdominal aorta and arises anterior to the body of the third lumbar vertebra a few centimeters above the aortic bifurcation into the common iliac arteries. A reverse curve catheter is often required to access it at angiography. (See Chapter 25 for further discussion of the inferior mesenteric artery and its branches, including the left colic artery, sigmoid arteries, and superior hemorrhoidal [rectal] artery.)
The testicular and ovarian arteries are paired visceral branches of the abdominal aorta that arise anterolaterally below the origin of the renal arteries. They pass inferolaterally, with similar paths in the abdomen but divergent ones in the pelvis. They descend into the pelvis along the anterior surface of the psoas muscles, (the right artery lies anterior to the inferior vena cava [IVC]), adjacent to the gonadal veins and ureters, and anterior to the iliac vessels. In the pelvis, the testicular arteries take a lateral course and enter the spermatic cord to continue into the scrotum, where they become tortuous and divide into several branches to provide the sole blood supply to the testes. The origin and course of the first part of the ovarian arteries are the same as those of the testicular arteries, but they take a more medial path in the pelvis. The ovarian artery travels through the suspensory ligament of the ovary (infundibulopelvic ligament) and provides branches to the ovary and fallopian tubes and small branches to the ureter. The artery then continues medially to the uterus and through the broad ligament, where it anastomoses with the terminal parts of the uterine artery. The ovarian arteries enlarge significantly during pregnancy to augment uterine blood supply. The most common variation in origin of the gonadal artery is from the renal artery, followed less often by the adrenal, lumbar, or even the iliac artery.
Lateral aortic branches include the middle adrenal (suprarenal) and renal arteries. The middle adrenal arteries are small and arise just above the renal arteries, one on either side of the aorta, opposite the superior mesenteric artery. They pass laterally and slightly upward over the crura of the diaphragm, where they anastomose with adrenal branches of the inferior phrenic and renal arteries and contribute to the vascular supply of the adrenal gland. As it travels to supply the right adrenal gland, the right middle adrenal artery passes posterior to the IVC. The origins of the middle adrenal arteries may be replaced by the celiac artery or superior mesenteric artery in 2% to 5% of patients.
The renal arteries, usually 4 to 6 cm in length and 5 to 6 mm in diameter, arise from the aorta just inferior to the origin of the superior mesenteric artery between the first and second lumbar vertebrae. The renal artery passes laterally and, after giving off the inferior adrenal artery, bifurcates into anterior and posterior branches that supply the renal parenchyma. (See Chapter 30 for further discussion of the anatomy of the renal arteries and renal vasculature.)
The posterior branches include the paired lumbar arteries and the median sacral artery. The lumbar arteries are usually four in number, although a smaller fifth pair may arise from the median sacral artery. They run laterally and posteriorly over the lumbar vertebral bodies and pass posterior to the sympathetic trunks and between the transverse processes of adjacent lumbar vertebrae to reach the abdominal wall. From this point onward, they demonstrate a branching pattern similar to a posterior intercostal artery, including segmental branches that supply the spinal cord. A small percentage of patients will have a lower anterior spinal artery, or artery of Adamkiewicz, arising from an L1 or L2 lumbar artery, which becomes clinically important when considering lumbar artery embolization. The lumbar arteries anastomose with one another, as well as with the lower posterior intercostal, subcostal, iliolumbar, deep circumflex iliac, and inferior epigastric arteries. These anastomoses may form the basis of collateral supply to the lower extremities in the event of distal aortic occlusive disease. Also, the initial segments of specific lumbar arteries may be hypoplastic with collateral flow from an adjacent artery.
The median sacral artery is small and arises from the posterior wall of the abdominal aorta, just proximal to its bifurcation. Alternatively, it may arise as a common trunk with the lumbar arteries or occasionally from the common iliac artery. It descends in the midline, anterior to the fourth and fifth lumbar vertebrae, and continues over the anterior surface of the sacrum and coccyx. There are anastomoses with the rectum, lumbar branches of the iliolumbar artery, and the lateral sacral arteries. It may be distinguished angiographically from the superior hemorrhoidal branch of the inferior mesenteric artery by its posterior location and lack of a terminal bifurcation.
The abdominal aorta bifurcates on the left side of the fourth lumbar vertebral body into the two common iliac arteries that supply the pelvis and lower extremities. Each is approximately 5 cm in length and 8 to 10 mm in diameter and passes inferiorly and laterally to divide into two terminal branches, the external iliac and internal iliac (hypogastric) arteries. (See Chapter 42 for further discussion of the Pelvic Vasculature.)
Inferior Vena Cava
The IVC, a single right-sided vessel in 97% of individuals, returns blood from all structures below the diaphragm to the right atrium of the heart. It is formed by the confluence of the two common iliac veins at the level of the fifth lumbar vertebra just to the right of midline. The IVC ascends anterior to the vertebral column through the posterior abdominal region on the right side of the abdominal aorta. Having reached the liver, the retrohepatic IVC resides in a groove on the posterior surface in the bare area of the liver and continues in a superior direction; it leaves the abdomen by piercing the diaphragm’s central tendon at the level of the eighth thoracic vertebra ( Fig. 19.7 ). During its course superiorly, the anterior surface of the IVC is crossed by the right external iliac artery, right gonadal artery, duodenum, pancreatic head, bile duct, portal vein, and liver, which overlaps and occasionally completely surrounds it. The supradiaphragmatic portion of the IVC pierces the fibrous pericardium and passes behind the serous pericardium to open into the inferoposterior part of the right atrium. In front of its atrial orifice is a semilunar valve, termed the eustachian valve or valve of the inferior vena cava , that is rudimentary in adults. However, it plays an important role during development by directing incoming oxygenated blood through the foramen ovale into the left atrium.