• Sensitivity and specificity of imaging findings are low (overlap those of GVHD)
• Ultrasound provides suggestive evidence of VOD; helps exclude other diagnoses (e.g., opportunistic infection)
Hepatosplenomegaly; ascites
Periportal and gallbladder wall edema
Hepatofugal flow on Doppler; ↑ resistive index (> 0.75)
Abnormal portal vein wave form
Small caliber hepatic veins
TOP DIFFERENTIAL DIAGNOSES
• Opportunistic infection, hepatic
• Graft vs. host disease
• Budd-Chiari syndrome
CLINICAL ISSUES
• Acute onset of painful hepatomegaly, jaundice, ascites within 3 weeks following hematopoietic or stem cell transplantation
• Occurs most frequently following HCT (affects 50-80% of recipients)
• Similar disease may occur following exposure to various toxic agents
Chemotherapy
Liver transplantation
• Treatment
Antithrombotic and thrombolytic medication
(Left) Complete obliteration of the central vein accompanied by centrizonal sinusoidal congestion is seen in venoocclusive disease (VOD). (Courtesy S. Kakar, MD.)
(Right) Endothelial swelling with subendothelial edema and fibrosis led to partial occlusion of the lumen of a small hepatic vein in venoocclusive disease. (Courtesy S. Kakar, MD.)
(Left) Axial T2WI MR in a 43-year-old woman with VOD following chemotherapy with FOLFOX for appendiceal carcinoma shows ascites and periportal edema , which are nonspecific findings. Liver biopsy showed sinusoidal congestion and fibrotic venules.
(Right) Axial contrast-enhanced T1WI MR in the same patient shows the ascites and periportal edema .









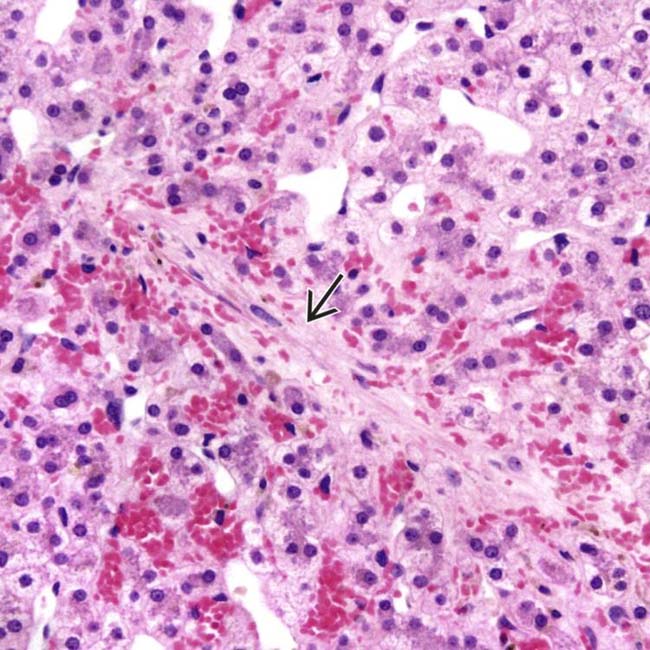
 accompanied by centrizonal sinusoidal congestion is seen in venoocclusive disease (VOD). (Courtesy S. Kakar, MD.)
accompanied by centrizonal sinusoidal congestion is seen in venoocclusive disease (VOD). (Courtesy S. Kakar, MD.)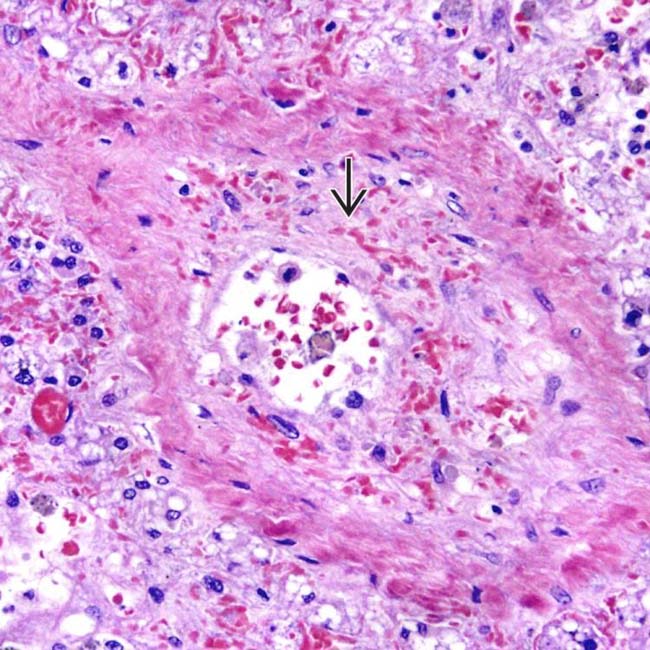
 led to partial occlusion of the lumen of a small hepatic vein in venoocclusive disease. (Courtesy S. Kakar, MD.)
led to partial occlusion of the lumen of a small hepatic vein in venoocclusive disease. (Courtesy S. Kakar, MD.)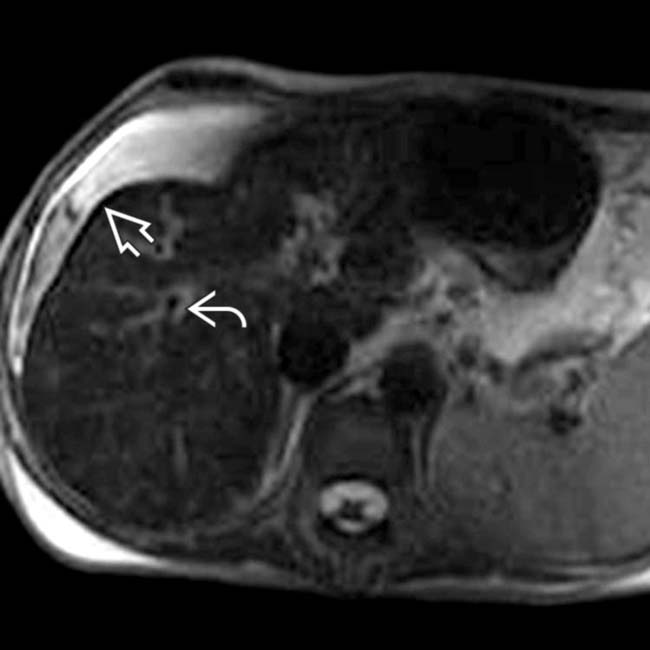
 and periportal edema
and periportal edema  , which are nonspecific findings. Liver biopsy showed sinusoidal congestion and fibrotic venules.
, which are nonspecific findings. Liver biopsy showed sinusoidal congestion and fibrotic venules.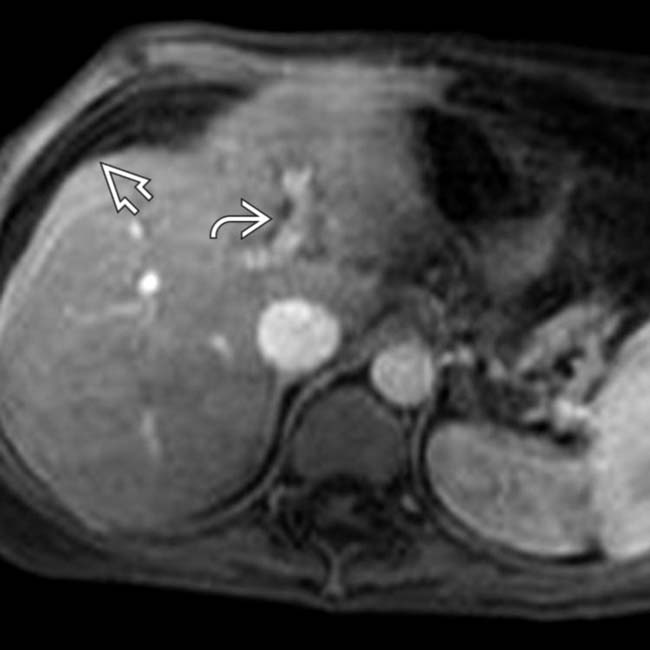
 and periportal edema
and periportal edema  .
.



