CHAPTER 49 Mastoidectomy
Epidemiology
Mastoidectomy is performed for suppurative disease of the middle ear and mastoid; cochlear implantation; access to the cerebellopontine angle, skull base, and petrous apex; labyrinthectomy; endolymphatic sac decompression; repair of facial nerve disorders; and cerebrospinal fluid leaks.
Clinical Features
A variety of mastoidectomy procedures can be performed, including simple, canal wall up (closed cavity or intact canal wall), canal wall down (open cavity), modified radical, and radical mastoidectomies. This chapter focuses on canal wall up and canal wall down mastoidectomies in the setting of chronic otitis media and cholesteatoma.
No prospective, randomized trials have been performed to indicate whether the canal wall up or canal wall down mastoidectomy is the definitive procedure for the treatment of cholesteatoma. Both procedures have been used successfully to treat cholesteatoma. The canal wall down approach has a lower incidence of residual or recurrent disease and can eradicate disease and preserve or restore hearing in a single operative procedure. It may also provide better intraoperative visualization of middle ear structures. However, the disadvantage of the canal wall down approach is generally a longer time for healing postoperatively and possible long-term local care of the mastoid cavity.
With the canal wall up approach, the normal anatomy is preserved, healing is quicker, and there is generally less need for long-term care of the operative site. The disadvantage of this technique is poorer operative exposure of disease extent, resulting in the need for greater surgical manipulation, longer operative time, and a higher incidence of residual or recurrent disease that may require further operative treatment.
Treatment
In a simple mastoidectomy, there is limited removal of mastoid air cells without entering the epitympanum or mastoid antrum. The ossicles cannot be directly visualized.
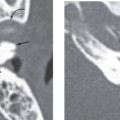
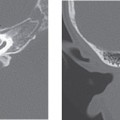
With the canal wall up mastoidectomy, there is resection of all mastoid air cells, the overlying cortex, and Körner septum with preservation of the posterior and superior walls of the external auditory canal (EAC). The resulting surgically created cavity, termed the “mastoid bowl,” communicates with the antrum and epitympanum, allowing direct visualization of the ossicles.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


