Craig Greben • Eric J. Gandras • Jason J. Naidich
Guido Guglielmi, the father of the detachable coil, stated that the development of this device was the result of the merging of three arts: electronics, neurosurgery, and interventional neuroradiology.1 The Guglielmi detachable coil (GDC) was invented in 1990 and revolutionized the field of neurointerventional radiology by allowing endovascular procedures to replace neurosurgical treatment in several cases over time. The ability to manipulate the coil and reposition it precisely into small, delicate aneurysms via an endovascular approach before deployment confers a significant advantage over pushable coils, which behave less predictably. The ability to pack coils densely into an aneurysm and successfully exclude it from the circulation represented a paradigm shift in the field of neurosurgery that has changed the way these lesions are managed.2
The success of the detachable coil in the field of neurointerventions led to the spread and cross-fertilization of this technology into the domain of peripheral embolization. Although the GDC was invented in 1990 and was used largely in the intracranial circulation, reports of its use for extracranial pathologies appeared shortly thereafter.3
GDCs detach from their delivery wire following the administration of an electric current. As a result, they can be fully pushed out of their delivery catheter but retracted completely if their position is unsatisfactory. In recent years, newer coil designs with different detachment mechanisms have been developed (Fig. 3.1). For example, the Interlock detachable coil (IDC) (Interlock Fibered IDC Occlusion System; Boston Scientific Corporation, Natick, Massachusetts) appeared on the market in the 1990s, and its early use for peripheral interventions was first described by Reidy and Qureshi4 in 1996. In contradistinction to the GDC, the IDC detaches through a mechanical release between the interlocking proximal end of the coil and the distal end of the pusher wire. As a result, the IDC can only be retracted if this interlocking domain remains within the delivery catheter. This can limit the precision of deployment and lead to inadvertent embolization requiring retrieval, as outlined by Reidy and Qureshi.4

DEVICE DESCRIPTION
The success of the GDC drove the development of other types of detachable coils, all of which remain attached to a wire until a release mechanism is used to achieve deployment. Electrical, mechanical, and hydraulic detachment mechanisms have all been used. This precise detachment allows for manipulation until a satisfactory position is achieved and minimizes the risk of migration or nontarget embolization. The physical properties that have been considered important in coil design include the stiffness and configuration of the device. Most current coil designs include a platinum alloy because it is biologically inert and has an optimal strength and rigidity to allow for conformational changes required for use in packing (Table 3.1). Because of the delicate nature of neurointerventional work, these coils have to be relatively soft to minimize complications. The design and configuration of the coil will determine its softness. These coils are manufactured with a stock wire wrapped around a mandril to produce a secondary structure, which usually has a helical configuration. A tertiary configuration can be constructed into the coil, which can include spherical and complex three-dimensional designs to optimize coil packing.5 These three-dimensional “framing” coils provide stability to the aneurysm wall. Softer two-dimensional “finishing” or “packing” coils can be placed within the framing coil to obliterate the space within the aneurysm with a safer margin during packing. These coils have historically ranged in size from 0.010 to 0.018 in in diameter and are meant to be deployed through a microcatheter, which serves to constrain the coil before deployment.

As with pushable coils, detachable coils work by encouraging stasis of flow and inducing thrombosis. Bare coils can fulfill this role, but blood can continue to flow through them, especially in high-flow regions or in the setting of coagulopathy. This is particularly true if the coils are loosely packed.6 Fibered coils have been developed to promote thrombosis, and the IDC is an example of this category of device. Other materials used to coat coils and promote thrombosis include polyglycolic acid (PGA) and nylon. Bioactive coils containing polylactic acid (PLA) have been developed to promote endothelialization and wound healing over the coil neck and mass.7 A further development in coil design has been the coating of platinum coils with a hydrogel polymer. These coils increase the density of packing by expanding in diameter once the gel is exposed to an ionic solution such as blood. The coils can swell between four and seven times the original diameter and thus increase packing density for the same length of coil deployed. This, theoretically, can lead to fewer coils required to exclude aneurysms, but this advantage is difficult to quantify in clinical practice.7,8 These hydrogel coils were first employed for peripheral interventions by Greben et al.9 who used them to exclude pulmonary arteriovenous malformations (AVMs) in 2005. The development of a peripheral hydrogel detachable coil (AZUR Peripheral HydroCoil Embolization System; Terumo Medical Corporation, Somerset, New Jersey) has led to further reports of their use for extracranial pathologies.10–12 These hydrocoils are predominantly used as finishing coils, as they must be detached within 3 to 5 minutes or else the expanded gel cannot be withdrawn or retracted back into the microcatheter delivery system. A 0.035-in hydrogel coil has been developed as well, which is considerably stiffer than the 0.018-in coils, with a larger volume of hydrogel associated with them. As with any detachable coil, the haptic experience of the stiffness is appreciated greatest at the junction of the coil and the delivery wire, or detachment zone, and this must be considered when attempting to place this segment of the coil into a confined, delicate space to avoid complications such as perforation.
TECHNIQUE
The ability to withdraw and reposition detachable coils before deployment affords a level of precision that may not be reliably achieved with pushable coils. This precision becomes more important in high-flow areas such as renal arteriovenous fistulas or aneurysms, pulmonary AVMs, and visceral aneurysms and pseudoaneurysms when the neck is close to the aorta or visceral branches. Detachable coils allow these challenging lesions to be treated safely while minimizing coil migration or inadvertent thrombosis of the native artery. There is also a risk of reperfusion from collateral circulation if lesions such as fistulas are closed too proximally. Occlusion at the level of the arteriovenous communication is necessary to prevent this from occurring. For larger high-flow fistulas, additional treatment strategies may be necessary such as balloon occlusion or double microcatheter, single guiding catheter technique that facilitates the building of a stable coil mass with the use of detachable coils.13 These techniques can also be employed in the treatment of wide-necked aneurysms, where detachable coils are safer to use than pushable coils in these challenging lesions. The risk of coil compaction and reperfusion or migration of the entire coil mass into the native vessel can be minimized with the addition of a stent to cage the mass.
CLINICAL APPLICATIONS
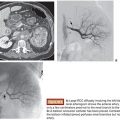
In general, detachable coils can be used for any indication where pushable coils are used. They are particularly useful for embolization when the delivery catheters are in tenuous positions or when the risk of coil migration is felt to be particularly high based on the pathology being treated (Figs. 3.2 and 3.3). However, they are significantly more expensive than pushable coils, which means that for more routine indications, the operator must consider the justification of the added cost. The time spent retrieving a migrated coil and the potential morbidity of this complication are intangibles that need to be weighed by the interventionalist. One method we employ to reduce cost is to use a combination of pushable and detachable coils; for the initial and completion coils, we use detachable coils with pushable coils in between. This permits precision during the procedure when the risk of coil migration is greatest.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


