Fig. 16.1
A 22-year-old male backstroke elite swimmer with posterosuperior impingement syndrome, a history of previous surgery for a SLAP tear and new shoulder pain and disability. (a) The fat-suppressed oblique coronal PD-weighted MRI shows re-tear of the labrum (SLAP type III) (open arrow) and a subcortical cyst in the humeral head (arrow). The T1-weighted MR arthrography (b, fat-suppressed oblique coronal; c, fat-suppressed axial; d, ABER position) confirms the presence of the cyst (arrows) and shows the SLAP lesion to better advantage (open arrows). In addition it shows a partial tear of the infraspinatus at the articular surface (small open arrow in b) and capsular thickening (solid arrow in d)
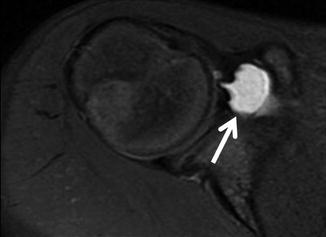
Fig. 16.2
An 11-year-old male elite swimmer with persistent shoulder pain despite rest. The axial fat-suppressed PD-weighted MRI shows subcoracoid bursitis (arrow)
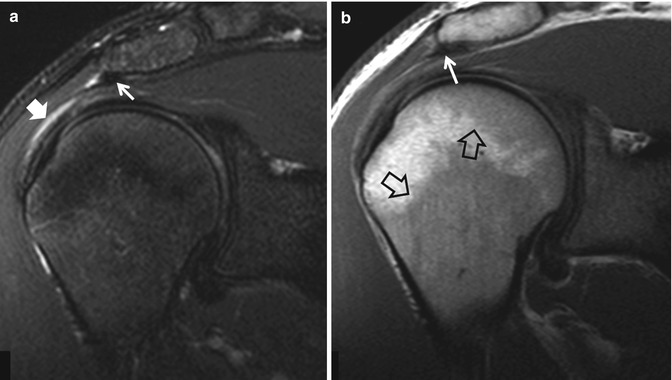
Fig. 16.3
A 19-year-old male elite freestyle swimmer, with a painful right shoulder. The oblique coronal fat-suppressed PD-weighted (a) and T1-weighted (b) MRI show subacromial bursitis (solid arrow), thickened coracoacromial ligament (thin arrows), and benign bone marrow hyperplasia (open arrows) due to increased hematopoietic demands

Fig. 16.4
The fat-suppressed oblique coronal PD-weighted MRI shows minor epiphysiolysis in a 12-year-old male elite butterfly swimmer with a painful right shoulder (arrows)
Medial and/or anterior knee pain is commonly seen in swimmers, especially breaststrokers (Rovere and Nichols 1985). Anterior knee pain may be more common in those athletes who have anatomic variations predisposing them to patella maltracking. Lateral pain in swimmers may be the result of a torn discoid lateral meniscus (Fig. 16.5a). Women show more knee pain problems than men.
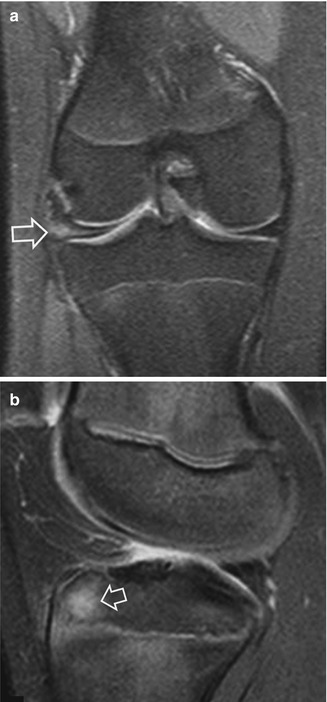
Fig. 16.5
(a) A 13-year-old female breaststroke swimmer with persistent lateral knee joint pain. The coronal fat-suppressed PD-weighted MRI shows a tear of a discoid lateral meniscus (arrow). (b) A 14-year-old elite breaststroke swimmer with persistent anterior knee pain. The fat-suppressed PD-weighted MRI in the sagittal plane shows a focal high signal intensity area corresponding to a stress reaction in the anterior tibial epiphysis (arrow)
The cause of knee pain in swimmers is not clear and synovitis, inflammation, and fibrosis of the synovial plica have been reported as related findings. Pes anserinus tendinitis or bursitis may result from repetitive valgus loads. The incidence of this symptom may be as high as 73 % (Kenal and Knapp 1996). Patellar tendinitis may result from repetitive quadriceps contraction seen in flutter kick in freestyle or during swimming pool wall push-off. Bone marrow edema on MRI, in keeping with stress reaction, may also be found (Fig. 16.5b). Its clinical value is strong if the imaging finding directly matches the point of tenderness. However, it is quite common to see MRI findings in asymptomatic elite athletes, such as infrapatellar fat pad edema (54 %), bone marrow edema (27 %), suprapatellar fat pat edema (19 %), and joint effusion (15 %) (Soder et al. 2012).
Overuse spinal injuries are common in swimmers. Low back pain is more common, with an incidence of up to 50 %, in butterfly and breaststroke swimmers. Lumbar strain may be related to twisting motions in flip-turning or when the body does not roll symmetrically during freestyle. Hyperextension of the lower back, inherent in all strokes but mostly in butterfly and breaststroke, induces load on the posterior structures, particularly with poor technique. Devices such as fins and pull buoys increase the degree of hyperextension. Thus, particularly in the end of the season and during the peak of competition, stress reactions and frank spondylolysis are common among adolescent elite swimmers (Fig. 16.6). Some cases of early disk degeneration and Schmorl nodes may be observed in elite swimmers; on MRI this finding is indistinguishable from early Scheuermann disease (Fig. 16.7) (Swischuk et al. 1998).
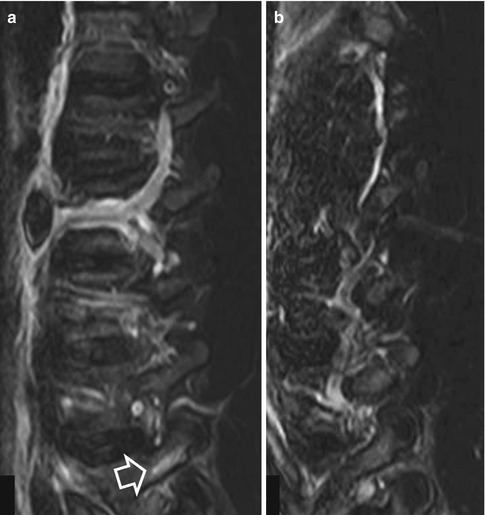
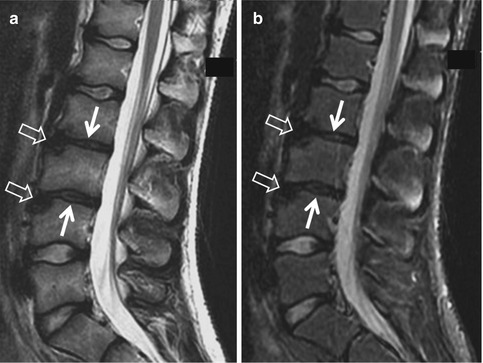
Fig. 16.6
A 15-year-old elite swimmer with stress reaction in the right L4 pedicle. (a) The right parasagittal STIR image shows bone marrow edema (arrow). (b) The left parasagittal image shows no abnormalities
Fig. 16.7
A 13-year-old elite breaststroke swimmer with persistent back pain. The sagittal T2-weighted (a) and STIR (b) MRI show early degeneration of the disks L2–L3 and L3–L4 (arrows) along with anterior herniation through the upper ipsilateral epiphyseal plate (open arrows). The lack of presence of multiple small extrusions within the central epiphyseal plates favors overuse and anterior Schmorl node formation rather than early Scheuermann disease
The use of swim fins during training induces stress in the ankle and foot. Stress reaction in the bone marrow and partial injury of the extensor retinaculum and tendons are common findings (Figs. 16.8 and 16.9). Contusion to the foot and sprains to the ankle may occur because of misplacement during a flip turn.
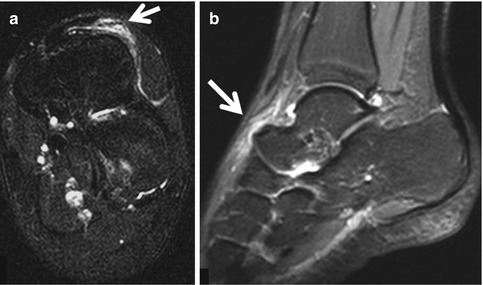
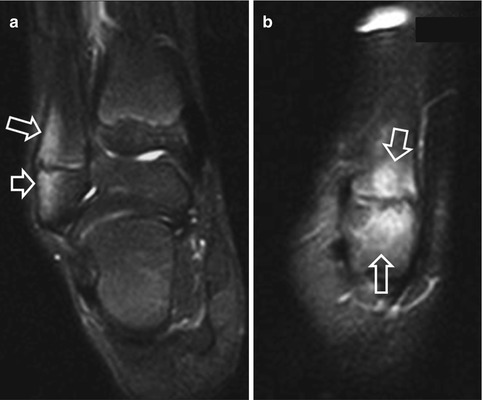
Fig. 16.8
A 14-year-old elite female swimmer reporting pain in the dorsal midfoot, exacerbated by use of swim fins. The oblique coronal fat-suppressed T2-weighted (a) and sagittal STIR (b) MRIs show edematous injury of the extensor retinaculum (arrows)
Fig. 16.9
An 11-year-old elite female swimmer reporting pain in the lateral ankle area, exacerbated by use of swim fins. The coronal fat-suppressed T2-weighted (a) and parasagittal STIR (b) MRIs show edematous changes within the bone marrow of the lateral malleolus, in keeping with stress reaction (arrows)
In a triathlon, cycling and running are mainly responsible for overuse injuries. With swimming, overuse usually afflicts the shoulder area. Triathletes use the freestyle stroke because it is the fastest among all styles and it allows lifting the head to confirm the proper direction, which is important in open-water swimming. Mechanical impingement is usually related to tendinopathy or the supraspinatus and biceps (Bales and Bales 2012). Ultrasound is the first-line examination. It is always useful to compare with the contralateral asymptomatic site as in many cases tendon degeneration occurs without any symptoms.
16.2.1.2 Recreational Swimming
Recreational swimming has a low incidence of severe musculoskeletal injuries. The most common injuries in our experience include bites, open wounds, sprains, strains, and bruises. In the north of the island of Crete, during the summertime, waves as high as 2 m may cause severe accidents, mainly in tourists who underestimate the risk. Bathers usually are swimming or playing in the sea close to the beach and may be caught and rolled by a wave and driven to the sea bottom at exactly the wave breakpoint. Closed cervical spine injuries occur when the bathers hit the sand; complex injuries of the cervical spine and face and skull with open wounds occur when they hit a rock. The injured bathers are either adolescents/young adults or middle aged and elderly, over 60, usually men. The former ignore the risk and the latter may lack physical ability or proper swimming technique and experience. The increased number of injured who show a neurological deficit in the latter group may be associated with preexisting cervical degenerative spondylosis. Similar profiles of injured bathers have been reported in a small series (Robles 2006). In accordance with the findings of that study, in our group of 7 patients, 6 sustained a hyperextension injury, which is comparable to the reported 75 %. Bathers is the standing position at the wave breakpoint land on their face. The injuries include the hyperextension teardrop fracture of the anteroinferior border of the vertebral body (Fig. 16.10), usually in older patients, and more severe injuries such as burst fractures, disk herniations, and locked facets in younger ones.

Fig. 16.10
A 42-year-old woman with an injury from hitting the sea bottom on her face. The sagittal T1-weighted (a) and STIR (b) MRIs show a hyperextension teardrop fracture of the anteroinferior corner of the C2 vertebral body (arrows) with prevertebral hematoma formation (open arrows)
16.2.1.3 Synchronized Swimming
Synchronized swimming is a hybrid of swimming, gymnastics, and ballet. This complex sport induces high demands on the athlete and often results in unusual injuries. Most partisans enter the sport as young girls at recreational level. The talented ones are chosen to train at a competitive level by the age of 13–15 years. Boosts and throws increase the risk of traumatic injuries including hematomas, contusions, sprains, acute tears of muscles and tendons, disk herniations, and fractures. Serious head injuries with post-concussive syndrome have also been reported (Mountjoy 1999). The “rocket split” move is responsible for acute groin, hamstring, and quadriceps strains. The 3 most common musculoskeletal overuse injuries encountered among elite and recreational synchronized swimmers are shoulder instability, lumbar pain, and patellofemoral syndrome (Weiberg 1986). Overuse may also result in tenosynovitis. Excessive pronation has been related to an otherwise rare entity, tenosynovitis of the extensor digitorum longus tendon (Fig. 16.11).
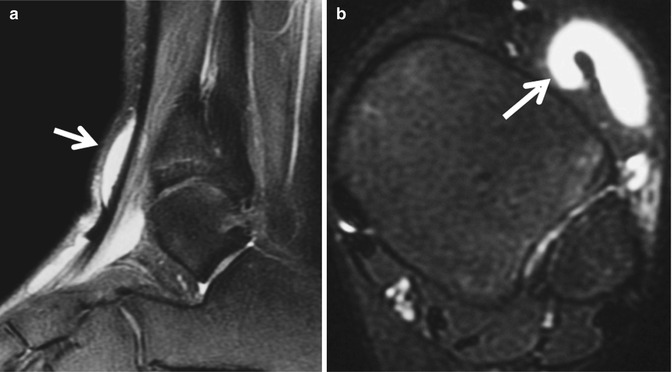
Fig. 16.11
An elite 12-year-old female synchronized swimmer tenosynovitis of the extensor digitorum longus tendon. The fat-suppressed sagittal PD-weighted (a) and axial fat-suppressed T2-weighted (b) MRIs show effusion (arrows) surrounding the tendon, due to overuse
Shoulder instability results from repetitive microtrauma and hypermobility of the joint. No imaging findings have been described in this group of injured athletes. Internal impingement may be the only clinical demonstration. As the problem is mainly muscular, there is good response to conservative treatment. In our database, a case of a HAGL lesion was attributed to a failed maneuver out of the water (Fig. 16.12).
Fig. 16.12
A 21-year-old female synchronized swimmer with a recent injury and persistent shoulder pain. The fat suppressed T1-weighted MR arthrographic image in the oblique coronal plane shows disruption of the humeral attachment of the inferior glenohumeral ligament, an HAGL lesion (arrow) and partial GAGL (solid arrow), with subsequent contrast extravasation along the medial humeral neck and under the scapula
Great flexibility in the lumbar and the rest of the spine is required in this sport which requires fast and repetitive arching movements such as the rocket move. Lumbar pain might result from facet dysfunction, poor pelvic posture, and overuse, together with poor muscular control. Spondylolysis is not as common as in other sports. Imaging will not show any findings in these athletes with lumbar pain. In our database, one elite child presented with a fatigue fracture of the sacrum (Fig. 16.13) and a second one presented with a stress reaction of the spinous process (Fig. 16.14).
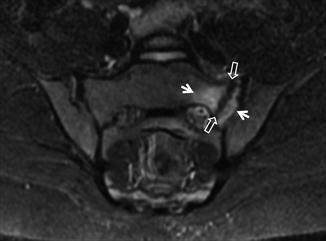
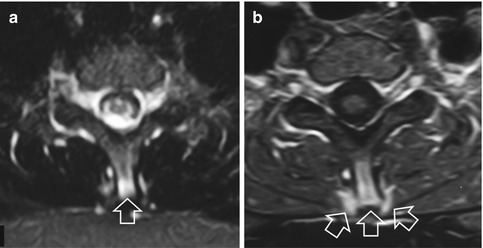
Fig. 16.13
A 10-year-old female synchronized swimmer with persistent low back pain but no history of recent injury. The oblique coronal STIR MRI shows a fatigue fracture of the left sacral wing (open arrows) surrounded by bone marrow edema (arrows)
Fig. 16.14
A 14-year-old female synchronized swimmer with stress injury in the cervicothoracic spine. The axial STIR (a) and fat-suppressed contrast-enhanced T1-weighted (b) MRIs show bone marrow edema and enhancement within the spinous process and the surrounding soft tissues (arrows)
The patellofemoral syndrome is mainly seen in the recreational rather than in the elite athlete. Chronic strain to the medial collateral ligament may coexist. The excessive “eggbeater” motion which enables the swimmer to raise her arms and body above the water is perhaps the main pathogenetic mechanism. This motion if combined with malalignment of the patella or vastus medialis oblique weakness may result in a painful medial or anterior knee joint syndrome.
16.2.1.4 Monofin Swimming
A monofin is typically used in fin swimming and free diving. It consists of a single surface attached to foot pockets for both the swimmer’s feet. The diver’s muscle power and swimming style and the type of activity the monofin is used for determine the choice of size, stiffness, and materials used. Technical monofin swimming at a competitive level induces significant stress in the lower spine. Disk herniations and Schmorl nodes may occur as a result of stress fracture of the epiphyseal plate (Fig. 16.15) (Paterakis et al. 2012).
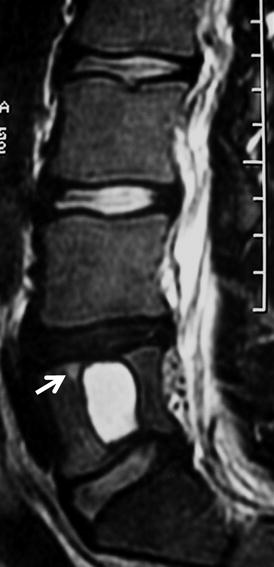
Fig. 16.15
A 16-year-old male elite swimmer, with sudden pain during monofin swimming due to a giant Schmorl node. The sagittal T2-weighted MRI shows the cystic nature of the lesion, the degeneration of the L4–L5 disk, and the reactive bone marrow edema (arrow)
16.2.2 Water Polo
Water polo is a contact sport that requires continuous swimming in rapid sprints up and down with abrupt changes of direction. Injuries include those resulting from overuse, like in swimming, and traumatic ones, like in wrestling.
Minor injuries occur frequently in water polo. Most of these do not require medical aid and include skin cuts, cut lips, and bruising, often in the supraorbital face, due to close contact with other players and high ball speed. One out of 5 elite water polo players have experienced some form of dental trauma, either from the high-speed ball or from close body contact. Severe injuries may occasionally happen, mostly in the face and head, and include fractures of the nasal bone and blow out of the orbits (Franić et al. 2007).
Low back pain is a common symptom in water polo players and is the result of intense rotational movements during throwing and passing the ball. Stress reaction and spondylolysis are included in the differential diagnosis of young athletes with persistent symptoms (Fig. 16.16). Acute nerve root compression in the lumbar region is usually the result of an acute disk prolapse. MRI should be applied in cases not responding to conservative treatment.

Fig. 16.16
A 15-year-old male water polo athlete with low back pain during the last 5 weeks. He reported 3.5 h of exercise for 5 times a week. The axial STIR MRIs show bone marrow edema in the right pedicle (arrow) and soft tissue edema (open arrow), in keeping with unilateral stress reaction
Water polo is associated with a high incidence of shoulder pain (24–80 %), mainly due to intense repeated overhead activity (Colville and Markman 1999; Webster et al. 2009). Pain usually reaches its maximum in the cocking phase of throwing with the arm abducted and externally rotated. Pain may also be exacerbated at maximum forward flexion of the joint in the catch phase of the freestyle stroke. Anterior pain usually suggests subacromial-subcoracoid impingement and posterior pain posterosuperior impingement. Female players have approximately double the rate of shoulder injury compared to men. The majority of shoulder soreness among female players is associated with less rest time between shots (Wheeler et al. 2013). Contact with opponents or the ball may result in dislocations and subluxations of the glenohumeral and the acromioclavicular joints. SLAP lesions result from repetitive biceps tension from overhead activity but are not usually seen in young athletes. Repetitive labral microinjuries might be demonstrated on MRI with intra-labral cysts (Fig. 16.17). Ganglion cysts may be demonstrated in elite athletes (Fig. 16.18). Shoulder instability and labral lesions, when clinically suspected, should be studied with MR arthrography. Rotator cuff tendinopathy and partial and full-thickness tears in the context of posterosuperior impingement are common in water polo athletes (38 %) (Fig. 16.19) (Giombini et al. 1997). Suprascapular nerve injury or entrapment is quite an uncommon injury. It may result from paralabral cysts extending to the notch, ganglion cysts within the notch, or previous glenohumeral dislocation. Clinically, there is deep posterior shoulder pain along with weakness of the shoulder girdle. MRI can show the cause and the aponeurotic process of the supraspinatus and infraspinatus muscles (Fig. 16.20).
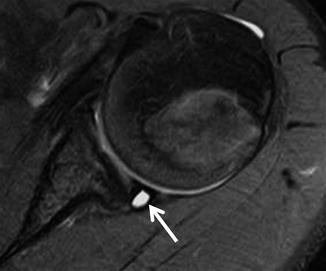
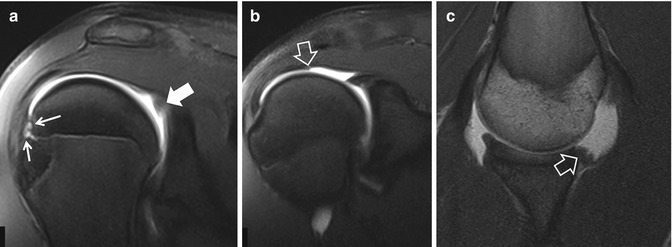
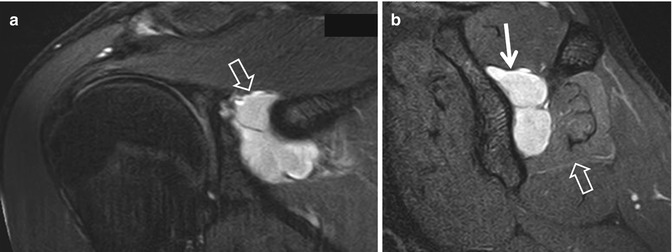
Fig. 16.17
A 15-year-old male water polo player with persistent shoulder pain particularly during throwing the ball, despite conservative treatment. The axial fat-suppressed PD-weighted MRI shows a labral cyst posteriorly (arrow)
Fig. 16.18
A 17-year-old male water polo athlete. The fat-suppressed oblique sagittal MRI shows a ganglion cyst located at the RC interval (arrow)
Fig. 16.19
A 15-year-old member of the youth national water polo team, with persistent pain at the onset of maximum effort for shooting. The fat-suppressed oblique coronal T1-weighted MR arthrographic images (a, b) show posterior labrum degeneration (arrow), subcortical microcyst formation (thin arrows), and irregularity of the undersurface of the supraspinatus tendon (open arrow), in keeping with posterosuperior impingement syndrome. (c) The T1-weighted MRI in the ABER position shows capsular thickening (arrow)
Fig. 16.20
A 24-year-old elite water polo player, with a history of 2 months of posterior shoulder pain and weakness. The fat-suppressed T2-weighted MRIs in the oblique coronal (a) and oblique sagittal (b) planes show a ganglion cyst within the suprascapular notch (open arrow in a, thin arrow in b) and edema within the infraspinatus muscle (open arrow in b) secondary to denervation
Elbow pain is a common complaint among water polo athletes. The differential diagnosis includes ulnar collateral ligament (UCL) injuries, valgus extension overload syndrome with olecranon osteophytes/posteromedial impingement, and osteochondritis dissecans (OCD) of the capitellum (Cain et al. 2003). Both MRI and ultrasound can be diagnostic in cases of UCL injuries. For the rest, MRI is the method of choice. CT can depict OD as well as intra-articular loose bodies. It has been suggested that valgus force applied to the capitellum, particularly in water polo goalkeepers, may be the cause of OD of the capitellum (Rod et al. 2013). MRI may show bone contusion to the posterior capitellum and partial tear of the anconeus muscle. In our series, OD was the most common injury among adolescent water polo players (Fig. 16.21).
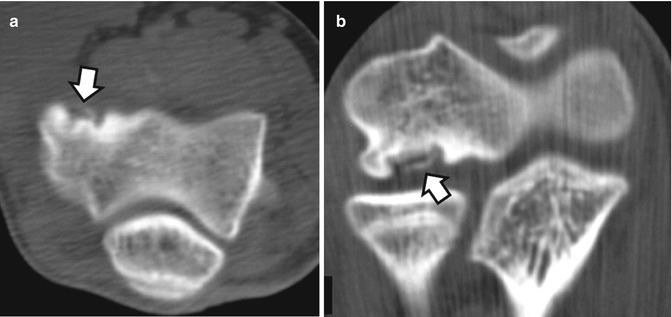
Fig. 16.21
A 15-year-old male water polo player with osteochondritis dissecans of the capitellum. The axial (a) and the coronal reconstruction (b) CT images show the complete detachment of the osteochondral lesion without displacement (arrows)
Stenosing tenosynovitis (de Quervain syndrome) of the first dorsal compartment is the most common tendinitis of the wrist in athletes using the upper extremities. Extensor carpi ulnaris tendinopathy is second to de Quervain in frequency but it may affect tendons in all dorsal compartments. Other commonly encountered acute injuries to the hand and fingers of water polo players include lacerations, dislocations of the interphalangeal and metacarpophalangeal joints and fractures of the phalanges and metacarpal bones (Hutchinson and Tansey 2003; Rettig 2003). Avulsion fracture of more than 40 % of the articular surface of the middle phalanx may need surgical treatment. Rupture of the collateral ligaments of the proximal interphalangeal joints may also be seen (Colville and Markman 1999).
Adductor muscle strains, demonstrated with groin pain, are a common injury in sports that involve sudden changes of direction as in water polo. It has been documented that leg work accounts for 40–55 % of the game, depending on the position played and game tactics. Water polo players seldom perform the breaststroke “whip kick,” but instead, the right leg rotates counterclockwise while the left rotates clockwise in the “eggbeater” kick unique to water polo. The rotation of the knee, with compression on the medial aspect of the joint, causes degenerative changes. Pain along or over the origin or insertion of the medial collateral ligament is typically an overuse syndrome from the chronic stress of the eggbeater kick, but mostly it is seen in young adult players.
16.2.3 Diving
Diving is the sport of plunging into water, usually headfirst, performed with gymnastic and acrobatic stunts. There are three forms of diving: recreational, competitive or platform, and underwater (scuba). Recreational activities are the mostly closely associated with severe injuries.
16.2.3.1 Recreational Diving
Sports account for 9–10 % of all spinal cord injuries (Ouzky 2002); 60–80 % of those injuries are caused by diving (DeVivo 1997; Aito et al. 2005; Barss et al. 2008). Amateurs usually do not master the proper technique. According to one study, spinal cord injury and diving-related trauma in general are very common in children aged 6–15 (Blanksby et al. 1997). Adult men aged under 35 are mainly at risk (Barss et al. 2008; Chan-Seng et al. 2013). In another study, the male to female ratio was 12:1; the majority of injured fell at the age group 15–29 and women were 12 years older (Amorim et al. 2011).
Any dive can result in death or severe lifetime disability. Misjudgment of the water depth, reckless behavior, and alcohol consumption are well-recognized risk factors (Korres et al. 2006). As a result, severe cervical spine injuries, with or without spinal cord involvement, are usually seen during summer months in Greece. The cervical spine is mostly affected (92 %), with 45 % of cases presenting with tetraplegia (Amorim et al. 2011). “Feet first-first time” programs have reduced the incidence of diving injuries in controlled and supervised areas. In our database, 28 spinal cord injuries with permanent disability were recorded in the last 7 years in recreational divers, all young men, after diving head first in shallow water (Fig. 16.22). No accidents occurred in younger persons; this may reflect that supervision of adolescents both in the Greek families and among tourists is an efficient preventative of such injuries.
Fig. 16.22
A 23-year-old male tourist, who dived into shallow water after alcohol consumption. The axial CT images show the fractures at the levels C5 (a), C6 (b), and C7 (c) (arrows). The sagittal (d) and coronal (e) CT multiplanar reconstruction images confirm the fracture dislocation of C7 (arrows) and the vertical fracture of the C6 vertebral body. (f) The sagittal T2-weighted MRI confirms the fractures and in addition shows a prevertebral hematoma (open arrow) and impact of the displaced fracture on the spinal cord (arrow), in keeping with the neurological compromise
Diving injuries are more disabling than those from motor vehicle accidents or falls, as nearly all involve the cervical region. In the majority of cases, C5 and C6 are the most commonly involved with fractures or fractures/dislocations and neurological injuries (Bailes et al. 1990). Few injuries may involve the thoracolumbar region, mostly L1 burst fractures type Denis B from axial load and flexion. This is mostly the result of unsupervised high jumping in the water, from young adult non-athletes who do not master any technique of diving (Kikuike et al. 2009). The mechanism of these kinds of injuries is related to the body posture prior to entering the water with buttocks instead of straight back and extended hips. CT and MRI are the methods of choice for assessing osseous and cord injuries respectively (Fig. 16.23).
Fig. 16.23
(a) Representation of the posture of those who are injured in the thoracolumbar spine, prior to entering the water from high jumping. A 23-year-old woman, who fell from a 16 m height onto the water, falling with the posture seen in a. The sagittal (b) and axial (c) CT images show the burst fracture of the T12 vertebral body with posterior displacement of the fracture elements causing central spinal canal stenosis (arrows). The sagittal T2-weighted (d) and STIR (e) MRIs show the abutment of the fractured vertebra upon the medullary conus (arrows), which seems intact in keeping with the good clinical status of the patient
16.2.3.2 Platform Diving
Few data exist on competitive or platform diving. Injuries are related to the 3 different phases of this sport. On takeoff, injuries include ankle sprains and tendinosis of the Achilles and posterior tibialis tendons. During flight, the divers are at risk for hitting the platform, resulting in contusions, lacerations, and fractures, mainly of the lower extremities. At the point of entry when diving from the 10 m tower, the speed may exceed 60 km/h and deceleration may reach 20G. Poor technique may result in landing flat in the water which is associated with injuries such as pneumothorax, rib fractures, tympanic drum perforation, and retinal detachment (Zimmerman 2007). At the elite level, the divers enter the water hands first, minimizing the splash. The latter is achieved either with both hands clenched into fists with one thumb wrapped in the other fist or with both hands open and flat with the wrists extended and radially deviated. Thus, hand and wrist chronic overuse injuries are common. They include bone bruises of the lunate, capitate, hamate, and distal radius; stress fractures of the scaphoid, radial styloid, and metacarpal bones; dorsal ganglion cysts; TFCC injury; flexor carpi ulnaris tendinopathy; scaphoid-lunate dislocations; growth plate injuries; scaphoid impaction syndrome; dorsal impaction syndrome; and radial styloid impingement syndrome (Rubin 1999; Zimmerman 2007). Taping the wrists is a protective measure against the dorsal flexion occurring at the entry point. Other sites of chronic overuse injuries in competitive divers are the spine and shoulder. The high deceleration forces may result in facet joint malfunction, paraspinal muscle strain, and spondylolysis. Triceps strains, due to handstand starting position of high-tower dives, are common and usually mild injuries (Wingfield 2004). We have seen 2 adolescent competitive athletes with medial meniscus bucket handle tears, which have not been previously associated with platform diving (Fig. 16.24).

Fig. 16.24
A 13-year-old female platform diving athlete, with acute knee joint pain. The fat-suppressed coronal (a) and sagittal (b) PD-weighted MRIs show the double PCL sign (arrows), in keeping with a bucket handle tear of the medial meniscus, confirmed and treated arthroscopically
16.2.3.3 Scuba Diving
Free diving or scuba diving is very popular at tourist destinations. Fatalities are quite common and have been associated with preexisting medical conditions such as ischemic heart disease (Sykes 1995). Drowning and death in free diving occur from lack of air, panic, injury by mistake from another diver, and entrapment in fishing nets. Decompression disorders in scuba diving may commence under the water but are clinically demonstrated after surfacing from the dive. These disorders include sickness, gas embolism, and barotrauma. Diving injuries and accidents can be significantly reduced with proper education (Degorordo et al. 2003). Imaging has a limited role in the diagnosis of such injuries.
16.2.4 Snorkeling
Snorkeling is the practice of swimming at the surface of the sea equipped with a mask and a short tube called a snorkel. Swim fins allow the swimmer to observe underwater for extended periods of time with relatively little effort. This kind of recreational activity is very popular among children and adolescents in the Mediterranean Sea and tropical resorts. Delayed-onset muscle soreness has been observed in young athletes, particularly at the beginning of holidays, and the diagnosis is clinical.
In middle-aged tourists who are participating in this kind of activity, sudden death may occur secondary to preexisting cardiovascular disease (Obafunwa et al. 1997).
16.3 Sports on the Water
16.3.1 Personal Watercraft and Powerboating Injuries
Personal watercraft, also known as Jet Ski crafts, are powered by a water jet. It has been shown that 9–30 % of the injured patients are younger than 16 years and one third of the injuries requiring care at a trauma center involve riders younger than 15 years (Hamman et al. 1993; Kim et al. 2003). Wide availability, easy accessibility, and lack of previous experience are the main causes of serious Jet Ski-related injuries. Most accidents involve collision between 2 vessels. Rectosigmoid perforation may result from hydrostatic injury following a fall off a craft (Gill et al. 2011). The head/face and neck followed by the spine and lower limbs are the most common locations of these injuries (Rubin et al. 2003; Carmel et al. 2004). Lower extremity injuries include hip and femoral fractures. The primary cause of death is blunt trauma, mainly to the central nervous system (Branche et al. 1997; Kim et al. 2003). Safety recommendations include minimum age of 16, operator training, operating regulations, and required helmet use. CT is the method of first choice for all serious injuries followed by MRI of the spine whenever neurological deficits exist. Children and adolescents are not allowed to operate Jet Skis by law. The few head injuries and femoral and rib fractures in our database were related to illegal use of a craft by an untrained person in late adolescence. Severely injured adults were mostly men between 18 and 25 years.
Powerboating is popular and is associated with increased risk for severe injuries and deaths. Most of the powerboating-related deaths are related to drowning and around 20 % to collisions. Age under 30 and alcohol consumption increase the risk for accidents.
The role of imaging in both watercraft and powerboating injuries is the same as for trauma patients in the emergency department.
16.3.2 Surfing
16.3.2.1 Windsurfing or Boardsailing
Windsurfing or boardsailing is a hybrid of surfing and sailing and is quite popular sport. Windsurfing was invented in 1969 by two Californians and is uses a board, a mast and a sail. The sport was included in the Olympic Games in 1984. Most injuries are acute due to impact with equipment, from jumping or from uncontrolled falls (Ullis and Anno 1984; Neville and Folland 2009). Equipment-related injuries result from contact with the boom (17 %), foot straps (17 %), mast (9 %), board (8 %), and fin with the lower extremities most commonly injured (44 %) (Nathanson and Reinert 1999). Overall, the injury incidence is low (1.5/person/year) including muscle/tendon strains and ligament sprains (Dyson et al. 2006). Injuries vary depending on the age and expertise of the athlete as well as the type of windsurfing and the specific weather and water conditions (McCormick and Davies 1988; Allen and Locke 1989). Windsurfing is associated with increased blood pressure and heart rate which is minimal in elite athletes but may be remarkable in dehydrated, unfit middle-aged weekend athletes or tourists, unfamiliar with the hypothermic environment of the seawater and unaware of their limitations. Close supervision is important in this respect.
Preadolescent and adolescent athletes present with injuries due to insufficient training and/or warming up. Beginners suffer from low back pain as they do not take sufficient advantage of the wind power (Fig. 16.25). Stress reaction and spondylolysis may occur. Not using a harness regularly, which attenuates the force transmitted through the spine, leads to lumbar compression. Beginners may also present with iliotibial band friction syndrome, due to poor technique which results in increased and asymmetric loading of the knee joints (Fig. 16.26). More severe injuries in beginners occur from beach starting, launching, or dismounting, particularly with heavy waves. Lacerations and abrasions result from contact with the board and its fin; muscular strains result from the effort to control the equipment at the wave break.

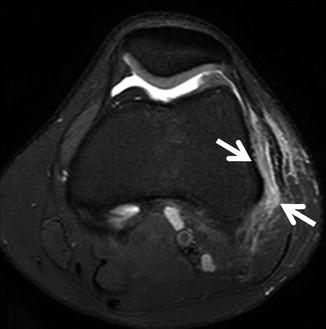
Fig. 16.25
(a) A 12-year-old elite swimmer and beginner in windsurfing with persistent low back pain. Lifting the mast and sail induces forces to biceps, back, thighs, and knees. (b) In the next season, the young windsurfer improved her technique and the loads on the back and thighs are symmetrical during tacking. (c) At the age of 15, the same athlete has upgraded the skills to the intermediate level, with proper use of the equipment balancing the power of the wind on the sail
Fig. 16.26
A 16-year-old female windsurfer with pain and tenderness in the lateral aspect of the knee joint. The axial fat-suppressed PD-weighted MRI shows edema in the soft tissues between the iliotibial band and the lateral femoral condyle (arrows) in keeping with iliotibial band friction syndrome
In athletes with moderate and advanced experience, low back pain and disk herniation results when light wind conditions create prolonged lordosis of the spine while pumping (Fig. 16.27). More severe injuries include rib fractures following a catapulted fall on the boom and fracture/dislocation of the elbow after falling on the board while the hand is still firmly attached to the boom causing hyperextension. Anterior shoulder dislocation may result from abduction and external rotation of the arm when the athlete is not able to keep the arms parallel to each other while using the back arm to pull the boom and sail against the wind (Figs. 16.28 and 16.29). A sudden forceful overload on a maximally contracted pectoralis major muscle of the posterior arm pulling the boom, resulting in a complete tear at or near the humeral insertion, is usually the result of poor technique (Fig. 16.30) (Dunkelman et al. 1994). At this level of expertise, overuse injuries are common. Lateral epicondylitis or “tennis elbow” due to repetitive stress on the arms, particularly under strong wind, is common (Figs. 16.28e and 16.31). Posterior impingement with “os trigonum” syndrome may occur following repetitive attempts at a water start, which uses the posterior ankle to raise the whole body weight with the help of the blowing wind (Figs. 16.28a, 16.32, and 16.33). Another overuse injury is anterolateral impingement due to repetitive microinjuries from twisting maneuvers or from falling with the feet trapped in the straps (Figs. 16.28c and 16.34). Foot injuries are very common (36.5 %) and include bruises, wounds, ligament ruptures, and muscle strains (Mettler and Biener 1991; Prymka et al. 1999). Achilles tendon tears usually occur in middle-aged and fit athletes. Tendonitis of the extensor digitorum longus tendon may result when the foot strap is used at the MTP level, which is preferred by advanced athletes for better board control (Hetsroni et al. 2006). Sprains and osteochondral injuries of the talus and fractures may occur if the strap moves to the midfoot level, trapping the feet during an unexpected fall or a badly designed jibe. Muscle contusions result from direct contact with the board and muscle strains from poor physical condition and improper warm-up (Fig. 16.35). In the author’s experience, going barefoot seems to be protective because the rider has a better feeling for the straps and board. “Tennis leg” with hematoma formation may occur at the end of a season due to fatigue of the calf muscles, after strenuous surfing and when dismounting, particularly with heavy waves (Fig. 16.36). Experienced athletes may incur fractures, osteochondral injuries, stress reactions, and labral tears, during demanding maneuvers, mainly. CT, MRI, and MR arthrography may be applied to the diagnosis of these lesions (Figs. 16.37 and 16.38).