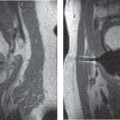
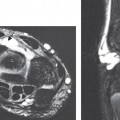
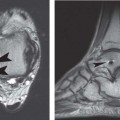
5 The Elbow MRI of the elbow has improved with the development of high-field systems and enhanced surface coil technology.1 Most centers image the elbow with the patient in the supine position and the arm comfortably positioned at the patient’s side, with the elbow in full extension. This position limits rotation of the proximal radioulnar joint with respect to the distal humerus and minimizes motion artifact compared with imaging the patient prone with the arm overhead. Axial, coronal, and sagittal images are obtained routinely.2 Most centers use a standard screening examination, consisting of an array of specified imaging planes and pulse sequences.3 In addition to standard T1-weighted and T2-weighted images, fat-suppressed T2-weighted and STIR sequences are extremely sensitive for detecting marrow and soft-tissue pathology by accentuating the increased signal of fluid and edema relative to the surrounding structures. These sequences are acquired with an FSE technique that produces the desired contrast in a fraction of the time needed for conventional T2-weighted sequences. Gradient-echo sequences are often used to evaluate ligaments and articular cartilage (see Chapter 14) and to delineate loose bodies in the elbow joint. However, these sequences should be avoided after elbow surgery (especially in the presence of metal hardware) because of the increased artifact inherent to the gradient-echo technique (see Chapter 1). A proton-density pulse sequence is occasionally used, often with fat suppression, and combines characteristics of T1-weighted and T2-weighted images. FSE pulse sequences have substantially reduced the length of examination, a great benefit for claustrophobic patients. Imaging parameters can be refined additionally for optimal cartilage visualization when indicated (see Chapter 14).4 MR arthrography is performed by injecting approximately 5 to 10 mL of diluted gadolinium contrast agent into the radiocapitellar joint from a lateral approach and acquiring fat-suppressed T1-weighted and T2-weighted images.5 Although somewhat controversial, MR arthrography of the elbow may help evaluate undersurface collateral ligament tears, capsular disruption, OCD, and intraarticular loose bodies. When investigating infectious, neoplastic, or synovial disorders involving the elbow, intravenous gadolinium is often used to evaluate for synovial hypertrophy or enhancement of pathologic tissues. Intravenous contrast is also useful for detecting soft-tissue abscesses, which show a thick enhancing wall surrounding the nonenhancing central fluid. Additional refinement of conventional MRI pulse sequences may eventually render these invasive techniques obsolete.6 Most patients with elbow trauma may be evaluated and treated adequately without the use of advanced imaging. However, for select patients, MRI may facilitate the diagnosis of suspected occult fractures, loose bodies, ligamentous injuries, and tendinous pathology. Conventional radiographs often are unrevealing in a patient presenting with elbow pain after acute trauma. In this setting, a joint effusion is often detected clinically, and an elevated posterior fat pad sign may be evident on conventional radiographs. Prospective studies in adults and children have shown that the presence of a posterior fat pad sign correlates with an occult fracture in more than 75% of patients.7,8 However, localizing the injury is a challenging endeavor, and patients often may be overtreated with immobilization in the absence of advanced imaging. MRI may be used in the setting of elbow trauma to localize and characterize osseous injury when conventional radiographs are unrevealing or equivocal. Fat-suppressed T2-weighted (or STIR) pulse sequences are the most sensitive images for detecting radiographically occult traumatic or stress fractures. Fractures show a linear pattern of signal change on T1-weighted (decreased signal) or T2-weighted (increased signal) images, whereas an osseous contusion often has a more nonspecific appearance (Fig. 5.1A). The most frequent site of occult fracture is the radial head; other sites, such as the lateral epicondyle or olecranon, are much less common.7 Radial head fractures may be accompanied by associated injuries that are most effectively detected by MRI, such as ligament or capsular disruptions, OCD, loose bodies, or capitellar bone contusions.9 Fig. 5.1 Osseous injury. (A) Bone contusions. A sagittal STIR image reveals high signal intensity within the capitellum and radial head, indicative of marrow edema (arrows). No discrete low signal fracture lines are evident. (B) Epiphysiolysis (Little Leaguer’s elbow). An axial STIR image of the right elbow showing diffuse high signal intensity within the medial epicondyle consistent with epiphysiolysis from repetitive valgus stress to the elbow (arrow). Part A is adapted with permission from Brunton LM, Anderson MW, Pannunzio ME, Khanna AJ, Chhabra AB: Magnetic resonance imaging of the elbow: update on current techniques and indications. J Hand Surg Am 2006;31:1001–1011. In children with a traumatic injury to the elbow and radiographic evidence of only a joint effusion, MRI is a sensitive and accurate modality for identifying or excluding an occult fracture.10 MRI reveals a broad spectrum of elbow pathology in this setting, including the following11: • Bone bruises • Ligamentous disruptions • Muscle injury MRI also may be effective in evaluating pediatric physeal injuries, especially in young children with poorly visualized ossification centers.12 Finally, MRI has a role in the detection of Little Leaguer’s elbow, a valgus stress injury in skeletally immature throwing athletes in which epiphysiolysis occurs at the medial epicondylar apophysis (Fig. 5.1B).13 The clinical manifestation of loose bodies within the elbow joint is typically pain with motion, often accompanied by mechanical symptoms, such as catching or locking. Loose bodies may originate from a traumatic shear injury to the osteochondral surface, synovial disorders, or OCD. The definitive treatment of symptomatic loose bodies is arthroscopic or open removal, but accurate diagnosis is imperative to prevent unnecessary surgery. Although conventional radiographs or CT may detect the presence of osseous loose bodies in the elbow joint, MRI is especially useful for detecting intraarticular cartilaginous or osteocartilaginous loose bodies. Loose bodies are found most commonly in the olecranon or coronoid fossae on T2-weighted images (Fig. 5.2). Osteophytes and synovial hypertrophy may mimic loose bodies on MRI images.3 The use of MRI for detecting loose bodies in the elbow has been disputed, and an overall low specificity and sensitivity, similar to that of conventional radiography, when compared with arthroscopic findings have been reported.14 MR arthrography may be effective in this setting, but it has not been studied adequately. The MCL is composed of the anterior, posterior, and transverse bundles. The anterior bundle is the most important stabilizer against valgus stress, and it can be divided into anterior and posterior bands. The anterior band is the primary restraint with the elbow in extension, and the posterior band is the primary restraint with the elbow in increasing amounts of flexion. MCL injuries have received tremendous attention because of their prevalence in throwing athletes of all ages and at all levels of competition.15 Accurate diagnosis of a full-thickness or partial-thickness tear of the MCL has important implications for treatment, as does the differentiation between MCL pathology and other causes of medial-side elbow pain, such as ulnar neuropathy, stress fracture, and flexor-pronator mass injury. Fig. 5.2 Axial (A) and sagittal (B) T2-weighted images showing loose bodies in the coronoid and olecranon fossae and in the trochlear ulnar joint (arrows on each). Adapted with permission from Brunton LM, Anderson MW, Pannunzio ME, Khanna AJ, Chhabra AB: Magnetic resonance imaging of the elbow: update on current techniques and indications. J Hand Surg Am 2006;31: 1001–1011. Fig. 5.3 MCL injury of the right elbow. (A) A coronal fat-suppressed T2-weighted image showing discontinuity (complete tear) of the MCL with surrounding edema and hemorrhage (arrow). (B) A coronal fat-suppressed T1-weighted arthrogram showing a partial tear of the MCL as a “T-sign” with leakage of intraarticular contrast at the undersurface of the MCL at its distal insertion on the sublime tubercle (arrow). Part A is adapted with permission from Brunton LM, Anderson MW, Pannunzio ME, Khanna AJ, Chhabra AB: Magnetic resonance imaging of the elbow: update on current techniques and indications. J Hand Surg Am 2006;31:1001–1011. Full-thickness tears of the anterior bundle of the MCL can be detected accurately by MRI. The MCL is seen on MRI as a vertically oriented, uniformly low signal intensity structure coursing between the medial epicondyle and the sublime tubercle on coronal images. The abnormalities detectable by MRI include ligament attenuation, redundancy, or discontinuity. Increased signal intensity often is found within and adjacent to the ligament on fat-suppressed T2-weighted images, indicating edema or hemorrhage (Fig. 5.3A).16 Concomitant findings, such as adjacent muscle edema and ulnar neuritis, are not unusual. MRI is less reliable for detecting partial-thickness tears, but the addition of intraarticular contrast may improve the sensitivity in this regard (Fig. 5.3B).17,18 The LCL complex of the elbow consists of four separate components: • RCL • LUCL • Annular ligament • Variable accessory LCL Injury to this complex from an acute elbow dislocation may lead to chronic mechanical symptoms or recurrent instability when early treatment is inadequate. Tears of the LUCL and RCL are common in acute elbow dislocations. Chronic insufficiency of the LUCL is believed to lead to posterolateral rotatory instability, which is often difficult to diagnose clinically.19 The ability of MRI to visualize tears of the LCL complex historically has been less dependable, especially in patients with chronic instability.20 One study of asymptomatic individuals revealed inconsistent MRI signal characteristics within the LUCL.21 Other investigators, however, have found MRI to be effective in detecting abnormalities of the LUCL in the setting of posterolateral rotatory instability when 3D gradient-echo and FSE sequences were used.22 Findings are similar to those seen in MCL injuries, with combinations of ligament attenuation, redundancy, and/or discontinuity evident on coronal or axial images (Fig. 5.4).12,16 MR arthrography in this setting has not been studied sufficiently to date.
 Specialized Pulse Sequences and Imaging Protocols
Specialized Pulse Sequences and Imaging Protocols
 Traumatic Conditions
Traumatic Conditions
Occult Fractures
Loose Bodies
MCL Injury

LCL Complex Injury
Biceps Tendon Injury


Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


