6 Ultrasound of the spleen and lymphatic system
The spleen – normal appearances and technique
Ultrasound appearances
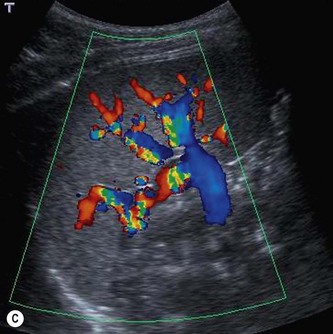
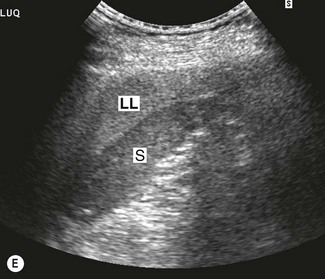
The main splenic artery and vein and their branches may be demonstrated at the splenic hilum (Fig. 6.1). The spleen provides an excellent acoustic window to the upper pole of the left kidney, the left adrenal gland and the tail of the pancreas.

Splenic variants
Splenomegaly
Enlargement of the spleen is a highly non-specific sign associated with numerous conditions, the most common being infection, portal hypertension, haematological disorders and neoplastic conditions (Box 6.1).
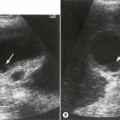
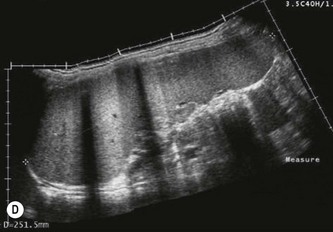
The spleen enlarges downwards and medially. Its inferior margin becomes rounded (Figs 6.1D, 6.2A) and it may extend below the left kidney and into the pelvis.

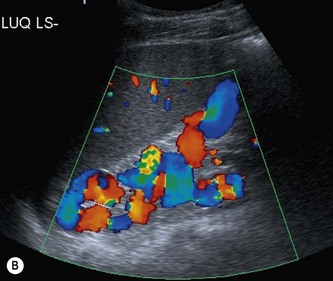
(B) Varices, in the form of a spleno-renal shunt, in portal hypertension.
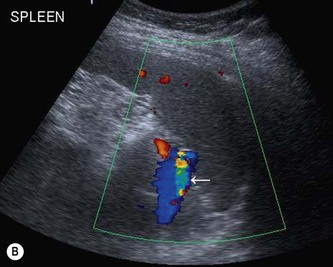
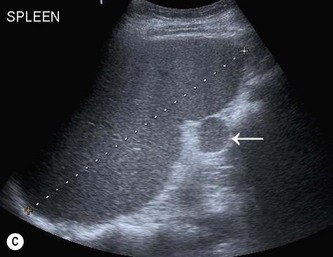
(C) A splenunculus (arrow) at the hilum of a mildly enlarged spleen.
Although the etiology of splenomegaly may not be obvious on ultrasound, the causes can be narrowed down by considering the clinical picture and by identifying other relevant appearances in the abdomen. Splenomegaly due to portal hypertension, for example, is frequently accompanied by other associated pathology such as cirrhotic liver changes, varices (Fig. 6.2A, B) or ascites (see Chapter 4).
Splenunculi
In around 10% of the population, a small accessory spleen, or splenunculus, may be located at the splenic hilum. These small, well-defined ectopic nodules of splenic tissue (Fig. 6.2C) rarely exceed 2 cm in diameter. Splenunculi enlarge under the same circumstances as those which cause splenomegaly, and may also hypertrophy in post-splenectomy patients.
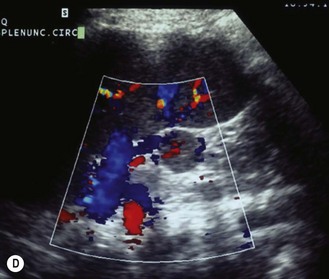
The importance of recognizing these lies in differentiating them from lymph nodes, left adrenal nodules or masses in the tail of pancreas. Colour Doppler may identify the vascular supply as being common to the main spleen (Fig. 6.2D).1
Pitfalls in scanning the spleen
Malignant splenic disease
Lymphoproliferative disorders
Lymphoma is the most common malignant disease affecting the spleen (Fig. 6.3). Malignant cells can infiltrate the spleen, lymph nodes, bone marrow and thymus and can also involve the liver, gastrointestinal tract, kidney and other organs. Approximately 3% of malignant diseases are lymphomas.
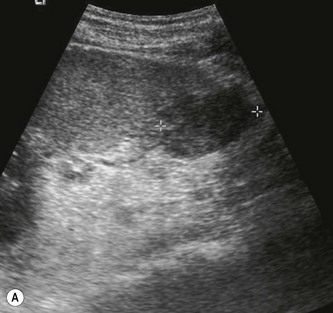



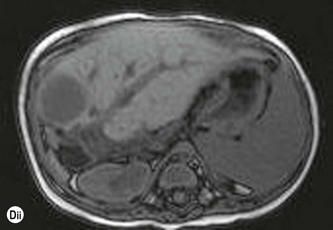
Fig. 6.3 • Lymphoma:
(B) Enlarged, coarse-textured spleen containing multiple tiny lymphomatous lesions.
(C) Extensive lymphadenopathy in the epigastric region.
Lymphoma is also associated with AIDS and infection with HIV has given rise to a broad spectrum of lymphomatous conditions which may be demonstrated on ultrasound and CT.2 These include masses in the liver, spleen, kidneys, adrenal gland, bowel and other retroperitoneal and nodal masses. In addition, the increased use of immunosuppression in transplant patients, and the increased survival in this group, has also been the cause of an increased incidence of immunodeficiency-related lymphoma known as PTLD (Fig. 6.3D) (see also Chapter 4).