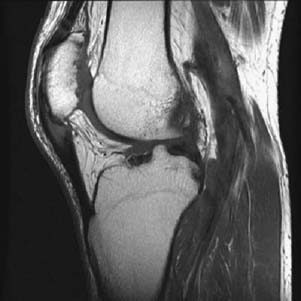
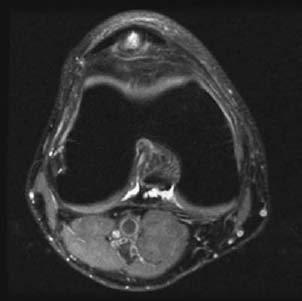
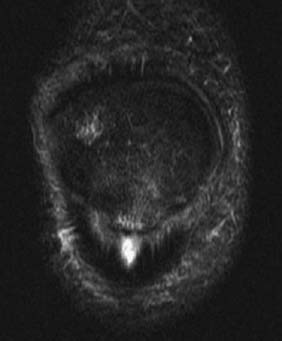
CASE 10 Anthony G. Ryan and Peter L. Munk A 20-year-old man presented with anterior knee pain, localized to the lower pole of the patella, focal tenderness at this site on examination, and moderate limitation of active knee extension secondary to pain. Figure 10A Figure 10B Figure 10C A sagittal T1-weighted image (Fig. 10A) shows focal tendon thickening of the proximal patellar tendon and intratendinous intermediate signal intensity. Focal low signal intensity is shown at the inferior pole of the patella. An axial proton density fat-saturated image (Fig. 10B) shows a focal “cone-shaped” focus of high signal intensity in the proximal patellar tendon. STIR sequence (Fig. 10C) shows a similar “cone-shaped” focus of high signal intensity at the same location. Ill-defined high signal is also demonstrated in the adjacent inferior pole of the patella. Jumper’s knee. In adults, the weakest link in the muscle-tendon-bone chain is the musculotendinous insertion. In adolescents, prior to epiphyseal fusion, the weakest point is at the tendon-epiphyseal or tendon-apophyseal junction. Jumper’s knee is the common name given to a partial tear of the patellar insertion of the patellar tendon, most commonly seen in younger athletes, including football players and track and field participants. Patellar tendinosis is thought to be caused by repetitive trauma resulting in microtears at the patellar tendon enthesis, on which background a partial or complete tear may more easily occur. Repetitive violent contractions of the quadriceps occur in “jumping” sports, basketball and volleyball being most commonly implicated. There is a spectrum of injury encompassing the following:
Jumper’s Knee
Clinical Presentation
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Extrinsic Factors
Pathophysiology
Clinical Findings
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


