CASE 19 Anthony G. Ryan and Peter L. Munk A 34-year-old amateur tennis player complained of pain on the inside of his elbow, which he noticed particularly when making a forearm smash. Point tenderness over the medial epicondyle was elicited on physical examination. Pain on resisted pronation of the forearm was evident. Figure 19A Figure 19B Figure 19C Figure 19D Ultrasound of the medial epicondyle and overlying soft tissues (Figs. 19A, transverse, and Figs. 19B, sagittal) reveals a focal area of hypoechogenicity within the common flexor tendon and edema at the musculotendinous junction. Coronal T2-weighted fat-saturated MRIs (Figs. 19C, elbow joint, and 19D, further posteriorly at the level of the olecranon) show diffuse high signal intensity overlying the medial epicondyle with laxity and partial discontinuity of the common flexor tendon. Medial epicondylitis. Ulnar collateral ligament tear. Also known as golfer’s elbow, pitcher’s elbow, or medial tennis elbow, medial epicondylitis is caused by degeneration of the common flexor tendon secondary to overload of the flexor/pronator muscle group arising from the medial epicondyle. Lateral epicondylitis, commonly referred to as tennis elbow, occurs more frequently than medial epicondylitis and is caused by degeneration of the common extensor tendon with or without the presence of tears. Most patients give a history of overuse. Degenerative tendinosis is common around the elbow, leading to a predisposition to tendon rupture. It was previously thought that a cycle of repetitive overuse led to recurrent and chronic inflammation, leading to the formation of scar tissue that is prone to further tears. However, repeated studies of tendons excised or débrided at surgery show no evidence of inflammatory cells but of degeneration only. Overuse syndromes produce repetitive microtrauma. Although typically thought of as an overuse syndrome secondary to tennis, lateral epicondylitis is actually seen more frequently in nonathletes. In the preadolescent age group, instead of a tendon tear, children are more likely to avulse the unfused medial epicondylar apophysis, this being the weak link in the muscle-tendon-bone chain. This is one variant of Little Leaguer’s elbow, the others comprising a stress fracture or delayed closure of the medial epicondyle apophysis. The patient typically complains of pain on the inside or outside (sometimes both) of the elbow, with point tenderness elicited directly over the affected epicondyle. Reproduction of the patient’s pain with resisted pronation (medial epicondylitis) or supination (lateral epicondylitis) is typical. Mild, moderate, or severe.
Epicondylitis
Clinical Presentation


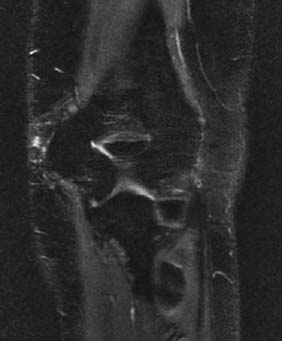
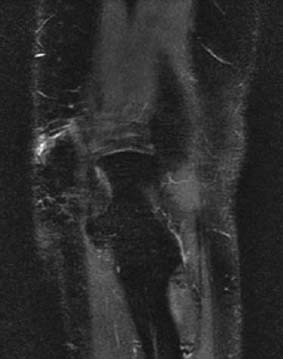
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
MEDIAL EPICONDYLITIS
LATERAL EPICONDYLITIS
Etiology
Pathophysiology
Clinical Findings
Stages of Disease
Complications
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


