- Conditions for acute radiation syndrome (ARS)
- Symptoms associated with the clinical syndromes of ARS
- Mean lethal dose
- Stages of ARS
- Bystander effect
Introduction
The effects of radiation are either stochastic or deterministic. Stochastic events are random events. They are thought to be initiated by radiation damage to a single cell, which is then passed on to future generations. The probability, but not the severity, of a stochastic event is a function of dose. The probability of a stochastic event increases with dose, but the precise relation is not known. In this way, stochastic effects are similar to the purchase of lottery tickets. Buying more tickets increases the chances of winning, but does not increase the amount of the prize. Cancer induction is one of the primary stochastic effects. Greater radiation exposure increases the chances of cancer but does not increase the severity of the cancer.
Children are about twice as sensitive as adults to stochastic effects, probably because they have a more rapid cell turnover during growth. They also have a longer lifetime after exposure to develop stochastic effects. Stochastic effects do not have a threshold because one cell could be damaged even at extremely low doses.
Deterministic effects result from injury to a population of cells leading to loss of tissue and organ function when sufficient cells are damaged. The amount loss is proportional to the radiation dose. Most organs can function with a loss of some functioning cells, and there is often a “threshold dose,” below which no loss of organ function is observed.
This chapter focuses on the deterministic effects of high doses of radiation to the whole body over a short period of time.
Acute Radiation Syndrome (ARS)
In the previous chapter, we discussed how different organs and tissues have different radiosensitivities, and that delivering the dose to a small area in a very short period of time is more damaging (e.g., to the skin) than spreading the dose out over a larger area, or a greater period of time. Radiation sickness, or ARS, is the result of a large dose of radiation delivered to the whole body in a short period (seconds to minutes) of time. The primary cause of ARS is the destruction of immature parenchymal stem cells in the affected tissues.
From the Center for Disease Control website, the required conditions for ARS are as follows:
Most of the data and examples we have regarding ARS are taken from the survivors of the Hiroshima and Nagasaki atomic bombings in 1945, as well as the first responders to the Chernobyl Nuclear Power Plant incident in 1986.
ARS is a collection of various deterministic effects that occur in a definite sequence. These effects, as discussed later, result in three distinct syndromes that occur in order, predictably with increasing dose. They are hematopoietic, gastrointestinal, and neurovascular syndromes. As their individual names imply, the syndromes are associated with which organ system is primarily affected by the received dose.
After a significant exposure that will result in ARS, there is a series of events referred to as the “phases of ARS.” The phases, discussed in more detail later, are prodromal, latent, manifest illness, and recovery or death.
Though most of the data regarding the stages of ARS come from Japanese atomic bomb survivors, some other clinical examples of ARS are as follows:
Mean Lethal Dose (LD50)
The mean lethal dose is defined as the amount of dose necessary to cause fatality in 50% of a population within a specified period of time. Because various clinical syndromes run their course in different time periods, the LD50 is assessed at different time periods. The time period in which death is assessed is denoted by a subscript denoting the number of days that has elapsed. For example, the LD50/30 is the dose necessary to kill 50% of the exposed population within 30 days, whereas the LD100/2 would be the dose necessary to kill the entire population within 2 days.
Being a statistical quantity, the LD50 varies between species and is not an absolute within the species, as it also depends on body weight and general health of the individual. The LD50 is only a guide in assessing the prognosis in any individual or animal. See Table 10.1 for an estimate of mean lethal doses for various species.
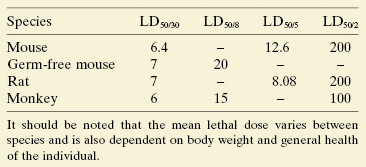
The LD50/30 for human whole body irradiation without medical intervention is approximately 5 Gy. However, as with any other clinical reaction, individual patients will respond differently to the same dose based on their overall health.
Clinical Syndromes of ARS
As discussed earlier, the effects of radiation depend on the dose received, and this holds for the clinical syndromes associated with ARS.
Hematopoietic Syndrome
When a person is exposed to about 1 Gy, the lymphocyte cell count will be reduced. The body will be more susceptible to infection. Early symptoms of such exposures mimic the flu, that is, loss of appetite, nausea, diarrhea, and vomiting. The chapter on whole body radiation treats the effects of decreased white blood cells following radiation exposure more completely. Figure 10.1 shows the radiation effects on white blood cell counts for ∼1–5 Gy.
Figure 10.1 White blood count (WBC) as a function of time after exposure. The figure shows plots of white blood cell count over time following exposure to different doses of ionizing radiation. These plots summarize data from the Chernobyl accident.
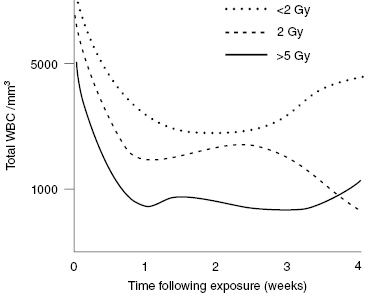
After a significant radiation dose (usually greater than 1 Gy), all components of the blood were adversely affected. Increases in dose result in an increased effect, and the effects are seen earlier. In the case of a whole body exposure from a radiation accident, the loss of white blood cells occurs just at a time when the body’s defenses against infection are most needed. Damage to the skin and intestine make the body particularly vulnerable to bacterial infection during the first 2 weeks following exposure.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


