Axial CT image at the level of lateral ventricles, sylvian fissure, and insular cortex.
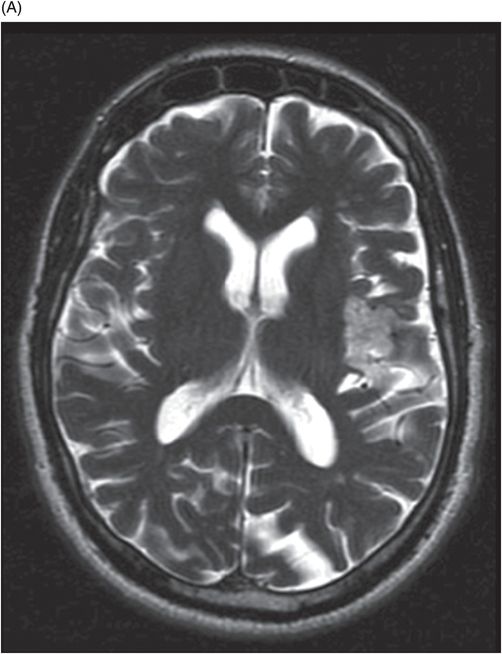
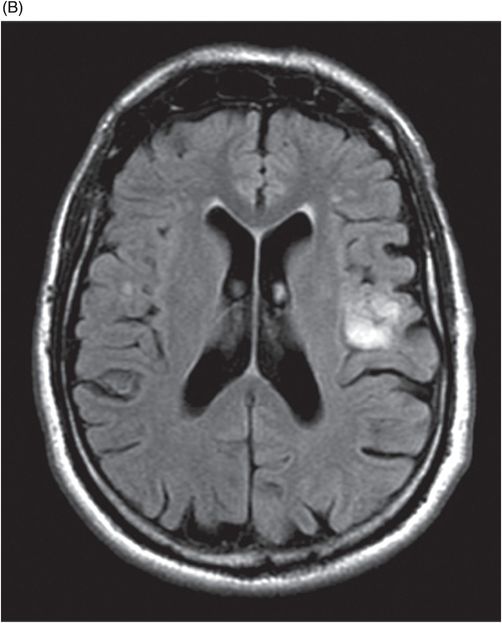
(A) Axial T2WI and (B) Axial FLAIR images at the level of lateral ventricles, sylvian fissure, and insular cortex.
Axial DWI at the level of lateral ventricles, sylvian fissure, and insular cortex.
Perfusion map image at the level of lateral ventricles, sylvian fissure, and insular cortex.
Intraparenchymal Epidermoid Cyst
Primary Diagnosis
Intraparenchymal epidermoid cyst
Differential Diagnoses
Arachnoid cyst
Dermoid cyst
Cystic neoplasm or metastasis
Abscess
Neuroepithelial cyst
Hydatid cyst
Imaging Findings
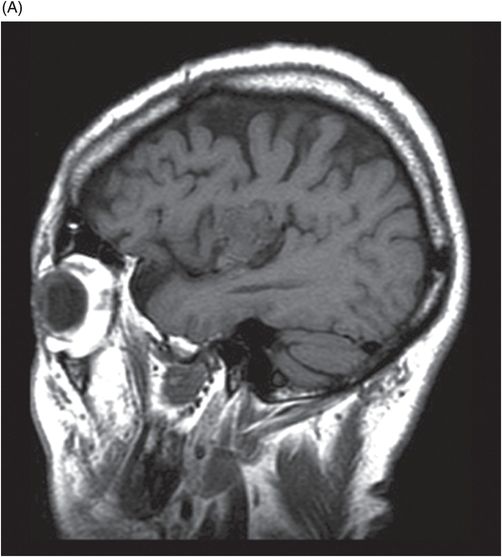
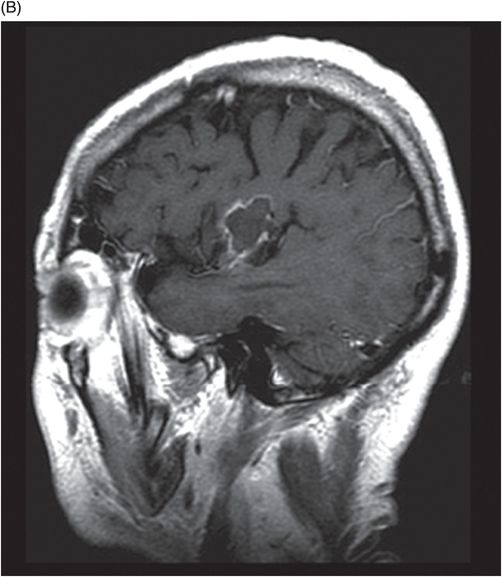
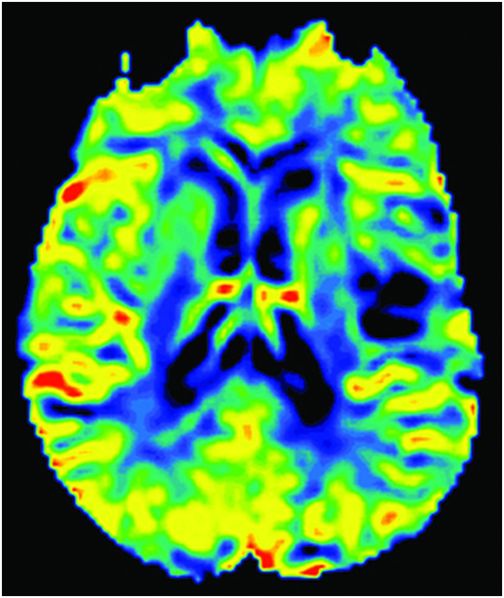
Fig. 100.1: Contrast CT axial image showed a lobulated hypodense and non-enhancing cystic lesion involving the left insular cortex and extending into the adjacent sylvian fissure. Few, small foci of peripheral calcification are noted. Fig. 100.2: (A) T2WI demonstrates an intra-axial lesion that appeared heterogeneously hyperintense on T2 and (B) FLAIR images with no evidence of vasogenic edema or significant mass effect. Fig. 100.3: DWI demonstrated diffusion restriction. Fig. 100.4: (A) T1WI sagittal images demonstrated a predominantly isointense lesion with few hyperintense foci that (B) showed peripheral enhancement. Fig. 100.5: Perfusion map shows hypoperfusion around the lesion.
Discussion
The extra-axial intracranial epidermoid cyst has classic imaging features: isodense to CSF on CT, isointense to CSF on T1WI and T2WI, mixed signal on FLAIR images and with restricted diffusion. Their much rarer counterparts, intraparenchymal epidermoids, are more difficult to diagnose accurately, as they usually lack this typical appearance.
The differential diagnoses include dermoid cyst, cystic neoplasm, neuroepithelial cyst, hydatid cyst, cystic metastasis, and brain abscess. Unlike epidermoid cysts, cystic neoplasms, metastases, and abscesses will often have enhancing rims and surrounding edema. However, neuroepithelial cysts, arachnoid cysts, and hydatid cysts can all share the CSF-like signal intensity of the epidermoid cyst. Nevertheless, unlike an epidermoid, a neuroepithelial cyst will have sharp and irregular borders, an arachnoid cyst will not demonstrate diffusion restriction, and a hydatid cyst will show the characteristic presence of a cyst and a pericyst. Dermoid cysts may cause restricted diffusion, but in contrast to epidermoids, they more commonly contain areas of fat, calcifications, and complex fluid.
Intraparenchymal epidermoid cysts are benign lesions arising from neuroectodermal epithelial cells. Their exact pathogenesis is still a subject of debate; the most popular theory suggests that they arise from epithelial rests that become sequestered in the primitive cerebral hemisphere during neural tube closure in the third to fifth week of embryogenesis. Intraparenchymal epidermoid cysts are rare, accounting for only 1.5% of intracranial epidermoid cysts and represent only 0.3–1.8% of primary intracranial tumors, with a female preponderance. Malignant transformation is exceedingly rare, although there have been case reports of transformation into squamous cell carcinoma, and of malignant melanoma arising within the lesion. Of the small number of intraparenchymal epidermoid cysts that have been reported in the literature, the most common locations in descending order of frequency are the frontal lobe, the temporal lobe, the parietal lobe, the occipital lobe, and the thalamus. Depending on the location of the tumor, various symptoms may arise, including headache, seizures, and hemiparesis.
On CT, intraparenchymal epidermoids are usually homogeneously hypodense with well-defined and lobulated margins. They can occasionally demonstrate cystic or calcified areas. Other non-calcified hyperdense areas can also be observed and are thought to reflect dense cystic contents or fat saponification with hemosiderin-laden macrophages. Mass effect can be present to a variable degree depending on the size of the lesion but perilesional edema is typically absent. Enhancement is usually absent, though rare cases of peripheral enhancement have been reported.
On MRI, intraparenchymal epidermoid cysts often exhibit iso- to slightly hyperintense signal intensity on T1WI and hyperintense signal on T2WI, though with more heterogeneity than typically seen in their extra-axial counterparts. Areas of high T1 and low T2 signal can be present, and are thought to represent a combination of proteinaceous material, debris, keratin, and incomplete calcification. Intralesional hemorrhage has also been reported. Hair-curled or whirlpool-like patterns are thought to represent desquamation of squamous epithelium. Diffusion-weighted imaging usually demonstrates heterogeneously hyperintense signal, with corresponding iso- or slightly hyperintense signal on ADC map. Minimal peripheral enhancement can be seen in some cases, making diagnosis difficult. Very rarely, restricted diffusion is absent, and in these circumstances, difficulties in establishing the diagnosis may arise.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


