CASE 102 Hema N.Choudur, Anthony G. Ryan, and Peter L. Munk Following a motor vehicle accident, this patient presented to the emergency department with cervical instability and neck pain. No neurological compromise was noted. Figure 102A Figure 102B Figure 102C The initial lateral radiograph (Fig. 102A) reveals a faint lucency across the neck of the odontoid with suspicious narrowing of the atlantoaxial distance. A helical CT with reformats (Fig. 102B, coronal, and Fig. 102C, sagittal) clearly shows the transversely oriented, mildly displaced base of the odontoid fracture. Type 2 odontoid fracture with associated narrowing of the atlantoaxial interval. None. Odontoid fractures account for 1 to 2% of all spinal fractures and for 8 to 15% of all cervical spine fractures. Displaced odontoid fractures (15 to 85%) can result in neurological deficit and nonunion if not promptly and appropriately treated. Of cervical vertebral fractures, C2 fractures are the most common. These fractures can result in very sinister complications due to cord compression; therefore, their prompt recognition and treatment are imperative. Most of these fractures occur following blunt trauma to the neck and motor vehicle accidents. A flexion loading force is the most common etiology, with anterior displacement of the dens. An extension loading force with posterior displacement of the dens occurs in a minority of cases. A rotational force can also occur. Following trauma to the dens, the bony break can be of three types: Type 1 These fractures are very infrequent and involve the tip of the odontoid. They occur in 5% of cases. These avulsion injuries result in an obliquely oriented fracture. Associated tear of the apical and alar ligaments can occur with instability of the detached fragment. Type 2 These fractures are the most frequent (60% of odontoid fractures), involving the base of the odontoid with or without displacement. Called body fracture, the fracture line passes above a horizontal line drawn through the upper border of the superior articular facets of the axis. These fractures result in severe complications, such as cord compression and respiratory distress as the atlas and occiput move as a unit. Identification of these fractures is therefore imperative. These fractures are also notorious for nonunion. Associated tear of the transverse ligament of the dens can occur and is well seen on MRI. Type 3
Odontoid Fracture
Clinical Presentation

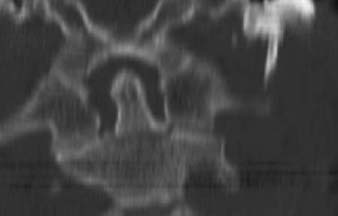

Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


