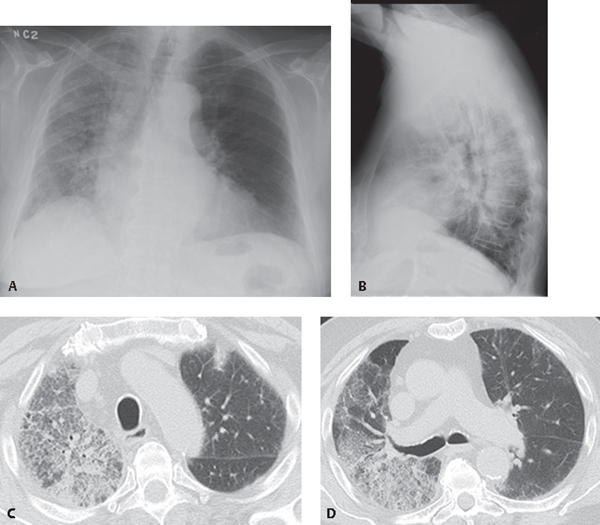
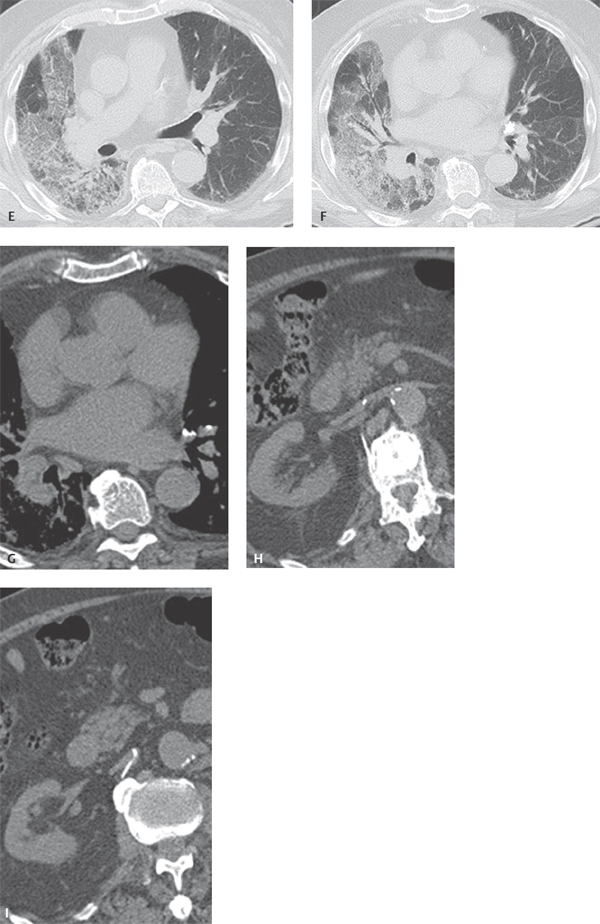
CASE 103 86-year-old man with new onset of dyspnea and non-productive cough developing five days following vertebroplasty of a symptomatic L1-L2 compression fracture. Respiratory failure developed over the following several days. PA (Fig. 103.1A) and lateral (Fig. 103.1B) chest radiographs demonstrate diffuse ground glass and reticular opacities throughout the right lung with associated volume loss. Unenhanced chest CT through the upper (Figs. 103.1C, 103.1D), mid (Fig. 103.1E), and lower (Fig. 103.1F) lung zones (lung window) reveal a diffuse “crazy-paving” pattern throughout the right lung with some foci of intervening normal lung. Mild bronchial and bronchiolar dilatation is seen in the affected lung. Subtle foci of ground glass and reticular opacities are present in the peripheral left lung. Unenhanced CT (mediastinal window) through the mid-thorax (Fig. 103.1G) and upper abdomen (Fig. 103.1H, 103.1I) shows high-attenuation polymethylmethacrylate in the anteromedial basal and lateral basal arterial divisions of the left lower lobe (Fig. 103.1F) and also emanating out from the L1 vertebroplasty site, with linear tracts extending into the paravertebral and extradural venous plexus into the right renal vein (Figs. 103.1H, 103.1I). Fig. 103.1 Fat Emboli Syndrome Complicated by ARDS Following Vertebroplasty • Acute Interstitial Pneumonia (AIP)/Acute Respiratory Distress Syndrome (ARDS) • Infection • Non-Cardiogenic Pulmonary Edema • Diffuse Alveolar Hemorrhage • Eosinophilic Pneumonia • Alveolar Proteinosis • Adenocarcinoma in-situ (formerly known as Bronchioloalveolar Cell Carcinoma [BAC])
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Various bacteria
Various bacteria
 Mycoplasma
Mycoplasma
 PCP/CMV
PCP/CMV
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine



