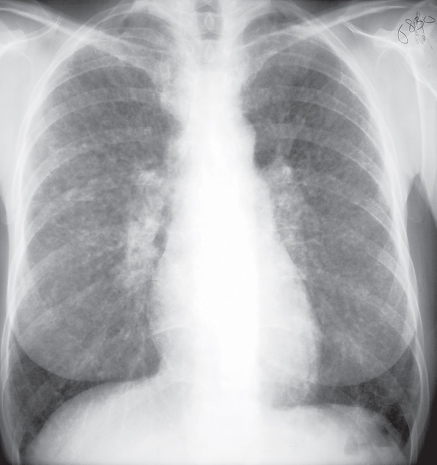
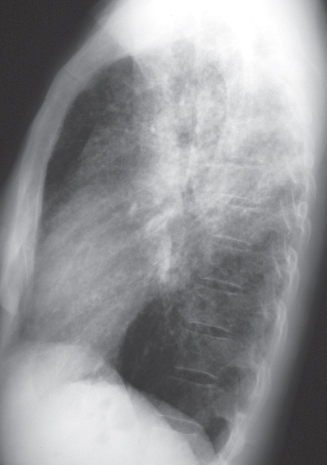
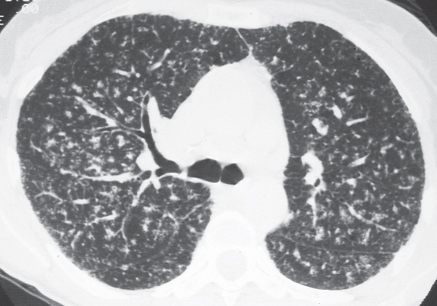
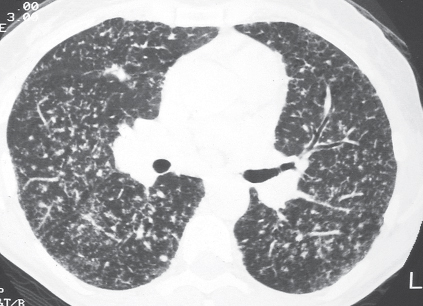
CASE 114 52-year-old woman with dyspnea and uveitis PA (Fig. 114.1) and lateral (Fig. 114.2) chest radiographs demonstrate profuse bilateral small pulmonary nodules most numerous in the upper and middle lung zones in association with symmetrical bilateral hilar lymphadenopathy. HRCT (Figs. 114.3, 114.4) reveals diffuse bilateral multi-focal micronodules distributed along perilymphatic areas, subpleural regions, interlobular septa, and bronchovascular bundles Sarcoidosis • Pulmonary Infection • Silicosis • Lymphoproliferative Disorder • Pulmonary Metastases Fig. 114.1 (Reproduced with permission from Miller BH, Rosado de Christenson ML, McAdams HP, Fishback NF. Thoracic Sarcoidosis: Radiologic-Pathologic Correlation. Radiographics 1995;15:421–437.) Fig. 114.2 Fig. 114.3 Fig. 114.4 Sarcoidosis is a systemic granulomatous disease that frequently affects the lung and the lymphatic system. The diagnosis is established based on typical clinical and radiologic findings supported by histologic evidence of non-caseating epithelioid granulomas in more than one organ. The etiology of sarcoidosis remains unknown. An abnormal immune-mediated response to a yet unidentified antigen has been postulated. Most affected patients are under the age of 40 years, with a peak incidence between 20 and 29 years. Annual incidence in the United States is 35.5 per 100,000 persons for African Americans and 10.9 per 100,000 for Caucasians. High disease prevalences are also reported in Swedes and Danes. Löfgren syndrome is an acute form of sarcoidosis characterized by fever, polyarthralgias, erythema nodosum and bilateral hilar lymphadenopathy. Heerfordt syndrome is the association of fever, parotid enlargement, facial palsy, and anterior uveitis. Lupus pernio is a chronic form of sarcoidosis typified by indurated plaques and raised discoloration of the central face and ears. Approximately 50% of patients with sarcoidosis are asymptomatic. Symptomatic patients may present with dry cough, dyspnea, chest pain, and hemoptysis. Non-specific symptoms are also reported, including constitutional symptoms, fatigue, weight loss, malaise, and fever. Pulmonary function studies may reveal restrictive abnormalities and decreased DLCO, but obstructive abnormalities can be seen with endobronchial sarcoidosis. Laboratory abnormalities include elevation of serum angiotensin converting enzyme (ACE), decreased blood serum CD4 to CD8 ratios, and hypercalcemia due to increased intestinal calcium absorption and activation of vitamin D by the sarcoid granulomas. Approximately 20% of patients develop pulmonary fibrosis, which may lead to pulmonary insufficiency and pulmonary hypertension.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Imaging Findings
Chest Radiography
Radiographic Staging System
 Stage 0: normal chest radiographs
Stage 0: normal chest radiographs
 Stage 1: hilar and/or mediastinal lymphadenopathy
Stage 1: hilar and/or mediastinal lymphadenopathy
 Stage 2: lymphadenopathy and parenchymal abnormalities (Figs. 114.1, 114.2
Stage 2: lymphadenopathy and parenchymal abnormalities (Figs. 114.1, 114.2Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine




