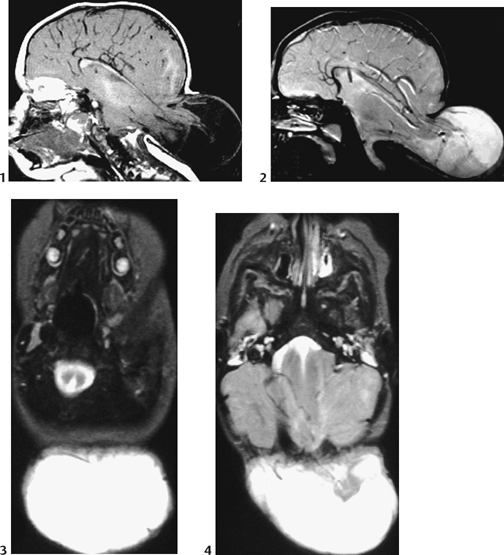
CASE 12 Infant girl presents with dysfunction of the lower cranial nerves, a large, posterior soft mass of the neck present since birth, and microcephaly. Figure 12A Sagittal MRI T1-weighted image (Fig. 12A1) shows a large posterior herniated sac filled with cerebrospinal fluid and cerebellum as well as posterior parts of the cerebral hemispheres. No subcutaneous fat is seen over it. The bony defect involves the infratentorial and supratentorial occipital bone, and therefore the posterior falx and tentorium as well. This implies that the dural venous sinuses are abnormal. Sagittal MRI T1-weighted image (Fig. 12A2) confirms the same anomalies, together with deformation of the course of the cerebral arteries. The axial T2-weighted images reveal the posterior split in the medulla (Fig. 12A3) and disorganization of the cerebellum (Fig. 12A4). The “heart-shaped” midbrain is tethered posteriorly to the sac (Fig. 12A4). Chiari III malformation Familial/ethnic occurrence similar to Chiari II, commonly associated with maternal dietary folate deficiency or methylene tetrahydrofolate reductase (MTHFR) mutations. Toxins such as Tripterygium wilfordii and arsenic also have been implicated.
Clinical Presentation
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Clinical Findings
Complications
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


