

CE-MRV MIP image.
Giant Arachnoid Granulation
Primary Diagnosis
Giant arachnoid granulation
Differential Diagnoses
Epidermoid cyst
Arachnoid cyst
Dermoid cyst
Calvarial hemangioma
Meningioma
Calvarial neoplastic lytic lesions
Venous sinus thrombosis
Imaging Findings
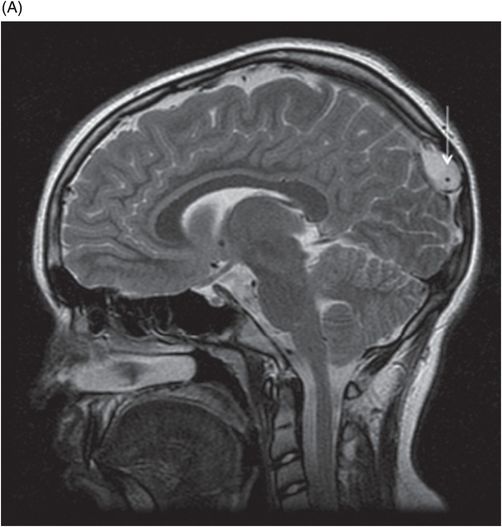
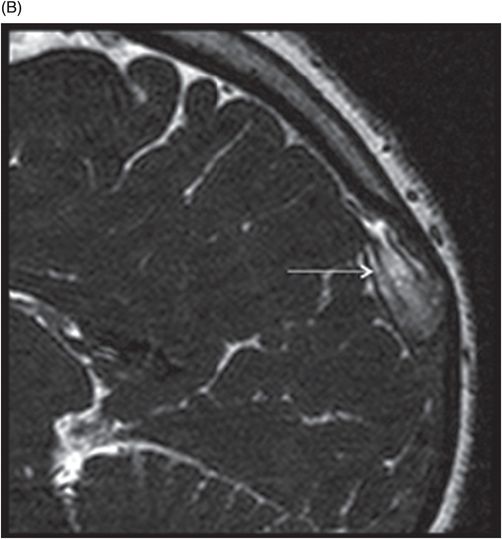
Fig. 128.1: (A) Contrast CT showed a hypodense filling defect (arrow) in the dorsal superior sagittal sinus with (B) scalloping of the inner table. Fig. 128.2: (A) T2 sagittal and (B) Heavily T2WI high-resolution images depict a linear flow void (arrow) which represents a vein coursing through the arachnoid granulation. Fig. 128.3: Axial source image of CE-MRV showed the enhancing veins traversing through the flow void. Fig. 128.4: CE-MRV MIP image showed the focal filling defect in the dorsal superior sagittal sinus.
Discussion
Although few entities can mimic arachnoid granulations, several lesion types should be considered in the list of differential diagnoses for arachnoid granulation. Intraosseous epidermoid cysts have similar signal intensity to CSF and can closely resemble arachnoid granulation. However, the absence of diffusion restriction and lack of complete suppression on FLAIR images confirm the diagnosis of arachnoid granulation. Arachnoid cysts also follow CSF signal intensity on all pulse sequences but heterogeneous enhancement as noted in arachnoid granulation aids in exclusion. The characteristic fat signal often noted in dermoid cysts also aids in ruling out differential diagnoses. Calvarial hemangioma, meningioma, and most neoplastic lesions show intense, solid patterns of enhancement, which are an uncommon trait of arachnoid granulations. Finally, venous sinus thrombosis can closely simulate arachnoid granulations and demonstrate varied density on CT and MRI images based on the stage of blood product degradation. Venous sinus thrombi are often described as having a sausage shape and can contiguously extend into the adjacent sinus. On the contrary, arachnoid granulations are round to oval and do not cross over into the adjacent sinuses. Sharp delineation and involvement of the inner table of the calvarium and a linear traversing vein characterize arachnoid granulations rather than a thrombus.
Arachnoid granulations, also termed pacchionian depressions, are expanded arachnoid villi that project into the dural venous sinus lumens, through which CSF is filtered into the central venous circulation. These are incidental findings, are found in two-thirds of the general population, are most often seen in patients greater than 40 years of age, and increase in frequency with age. They are most commonly found in the transverse and posterior superior sagittal sinuses, but they are also frequently seen in the sigmoid, sagittal, and straight sinuses. They often are located in close association to the dural venous sinus, along penetrating veins, and are postulated to be weak areas within the dura through which these villi can project into the sinus lumen.
The arachnoid granulation meningothelial lining is thin at the base and absent at its apex. The internal network is supported by collagenous soft tissue filled with CSF flowing from the subarachnoid space. Cerebrospinal fluid migrates to the granulation apex, which is lined by arachnoid cells, and is thought to be actively transported into the venous circulation. Larger granulations are more likely to contain fibo-collagenous tissue and internal veins.
Normally, arachnoid granulations range from 5 to 15 mm. There is no common consensus in the literature regarding the size criteria; however, arachnoid granulations greater than 10–15 mm are termed giant arachnoid granulations. Some authors refer to arachnoid granulations as giant when they are large enough to occupy the entire lumen of the sinus and result in focal dilatation. Giant granulations as large as 2.4 cm have been reported in the literature. They may grow to occupy and dilate the dural sinuses or expand the outer table, mimicking osteolytic lesions. They are typically asymptomatic, with rare exceptions, when they can present with headache and features of pseudotumor cerebri if there is a pressure gradient across the giant arachnoid granulation resulting in venous hypertension. Rarely, they can cause partial sinus occlusion. On imaging, arachnoid granulations are single or multiple ovoid lesions and typically appear as focal osseous pits in the inner table of the calvarium. Computed tomography images show a well-circumscribed, discrete filling defect in the dural venous sinus with CSF density.
Diagnosis is often established on MRI, where conventionally arachnoid granulations follow CSF/clear fluid signal intensity on T1 and T2WI and typically do not enhance. Often, linear enhancement is noted in large granulations, which is usually due to a traversing vein. Few exceptions to this rule have been demonstrated in the literature where on FLAIR, granulations can be hyperintense, possibly due to pulsation artifact from the adjacent sinus or altered CSF flow in approximately 9–10% of cases. Diffusion restriction changes can be seen in large arachnoid granulations and are presumed to be due to stromal collagenous tissue.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


