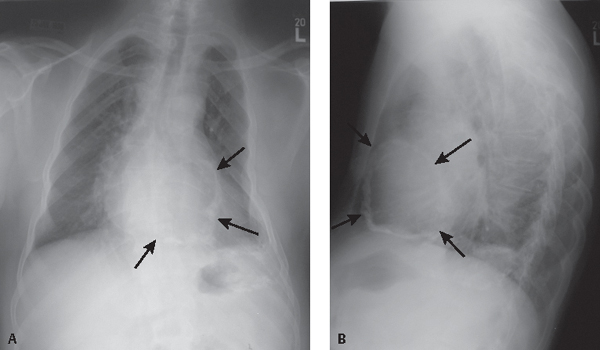
CASE 141 61-year-old woman with remote history of tuberculosis, but no current respiratory complaints PA (Fig. 141.1A) and lateral (Fig. 141.1B) chest X-rays reveal thick, chunky, amorphous calcifications over most of the heart’s surface (arrows) and along the atrioventricular groove. The left chest wall is deformed secondary to remote trauma. Amorphous pleural calcifications are seen in the posterior and lateral left thorax from a remote traumatic hemothorax (calcific pleuritis). Note the asymmetric left apical pleural fibrosis. Pericardial Calcifications—Secondary to Remote Tuberculous Pericarditis, Non-Constrictive • Pericardial Calcifications from Other Causes of Remote Pericarditis • Myocardial Calcifications Fig. 141.1 Normal pericardium is composed of two layers: a tough fibrous parietal pericardial layer and a smooth visceral pericardial layer. Approximately 20–50 mL of transudative fluid is normally present between these two layers, which minimizes friction during the cardiac cycle. Inflammation of the pericardial layers is called pericarditis. Acute and subacute pericarditis may be associated with fibrin deposition along these layers and concomitant pericardial effusion. Subsequent organization results in fibrosis, scarring, and sometimes calcification, most often of the parietal pericardium. Thin, linear, “eggshell calcifications” are more often associated with viral and uremic pericarditis. Shaggy, thick, amorphous calcifications are more often associated with tuberculous pericarditis. Calcium deposits tend to be most obvious in the atrioventricular groove, where more fat is usually found. The thickened, fibrotic pericardium may impair normal late diastolic ventricular filling. Approximately 9% of patients with acute pericarditis develop constrictive physiology. Those clinical entities associated with acute pericarditis are likewise responsible for the development of constrictive pericarditis. These most commonly include idiopathic (presumably viral) (e.g., coxsackievirus A and B, adenoviruses), tuberculosis, cardiac surgery–related, and radiation therapy–induced. Less common causes include neoplasia, uremia, various connective tissue disorders (e.g., rheumatoid arthritis, systemic lupus erythematosus, scleroderma), drug-induced (e.g., procainamide, hydralazine), and myocardial infarction. Calcific pericarditis without constriction is often asymptomatic and found incidentally on chest exams. However, it can be associated with constrictive pericarditis,
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


