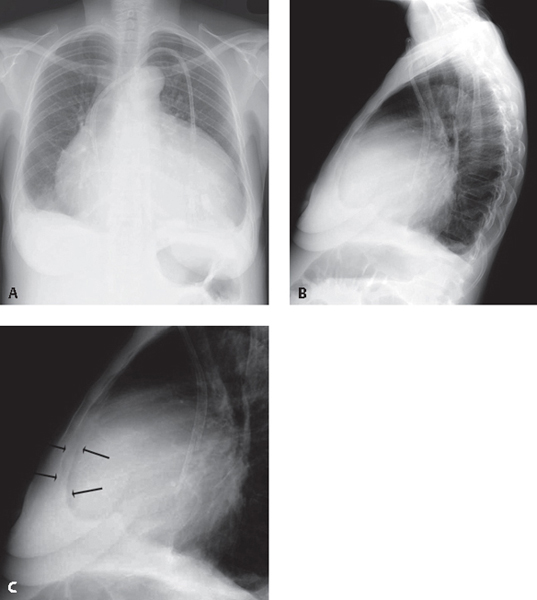
CASE 142 40-year-old woman with long-standing uremia presents with increasing shortness of breath PA (Fig. 142.1A) chest X-ray reveals an enlarged cardiomediastinal silhouette with an increase in the transverse diameter but no increase in its height, and straightening of the upper mediastinal borders, creating a globular or water bottle morphology (water bottle sign). The vascular clarity is slightly diminished and bilateral pleural effusions are present, right greater than left. Lateral (Fig. 142.1B) exam also shows globular enlargement of the cardiomediastinal silhouette and separation of the outer retrosternal and inner epicardial fat lines—fat pad or Oreo cookie sign). This latter sign is seen to better advantage on the coned-down lateral view (Fig. 142.1C) (arrows). Pericardial Effusion Fig. 142.1 • Global Cardiomegaly—Cardiomyopathy The pericardium consists of two layers. Visceral pericardium is attached to the surface of the heart and the proximal great vessels. Parietal pericardium forms the free wall of the pericardial sac. The sac normally contains 20–50 mL of fluid. The most common cause of pericardial effusion is myocardial infarction with left ventricular failure. Fifty percent of patients with chronic renal failure develop uremic pericarditis. Coxsackievirus group B, Staphylococcus, and Haemophilus influenzae are common infectious agents associated with pericardial effusion. Today, tuberculous pericarditis is unusual except in the HIV-AIDS population, in which pericardial effusion of any etiology is a poor prognostic sign. Increased volumes of pericardial fluid and alterations in the composition of normal pericardial fluid may occur in the setting of numerous diseases (Table 142.1).
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


